

A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals
- PMID: 15729062
- PMCID: PMC1356978
- DOI: 10.1097/01.sla.0000154120.96169.99
A systematic review of strategies to improve prophylaxis for venous thromboembolism in hospitals
Abstract
Objective: To assess the effectiveness of different strategies for increasing the uptake of prophylaxis for venous thromboembolism (VTE) in hospitalized patients through a systematic review of the literature.
Methods: Literature databases and the Internet were searched from 1996 to May 2003. Studies of strategies to improve VTE prophylaxis practice were included. Studies where no policy or guideline was implemented or where the focus of the study was not VTE prevention were excluded.
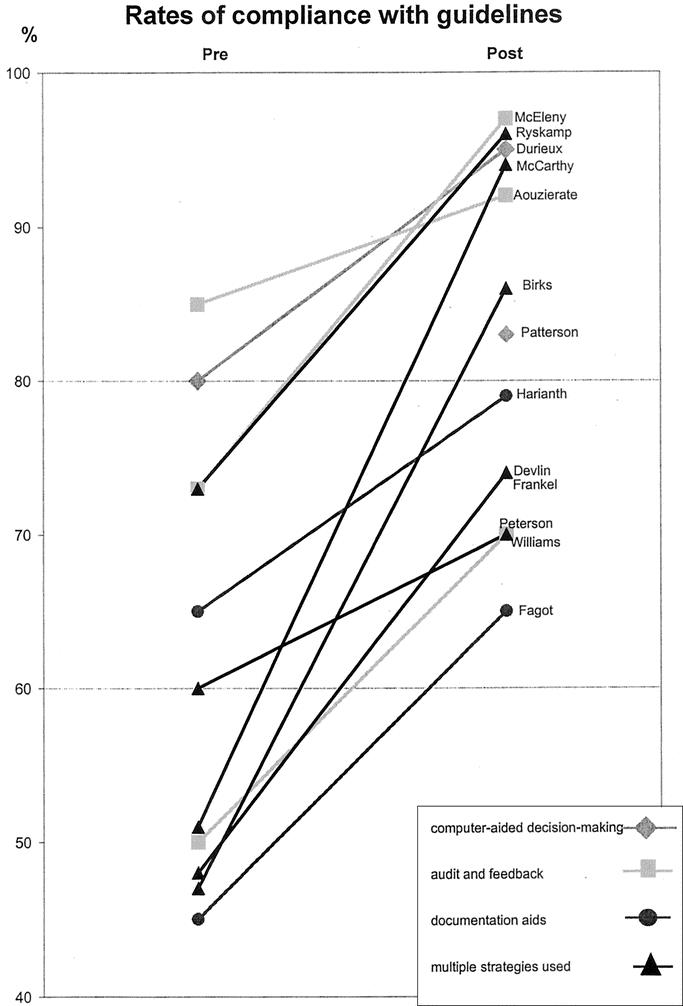
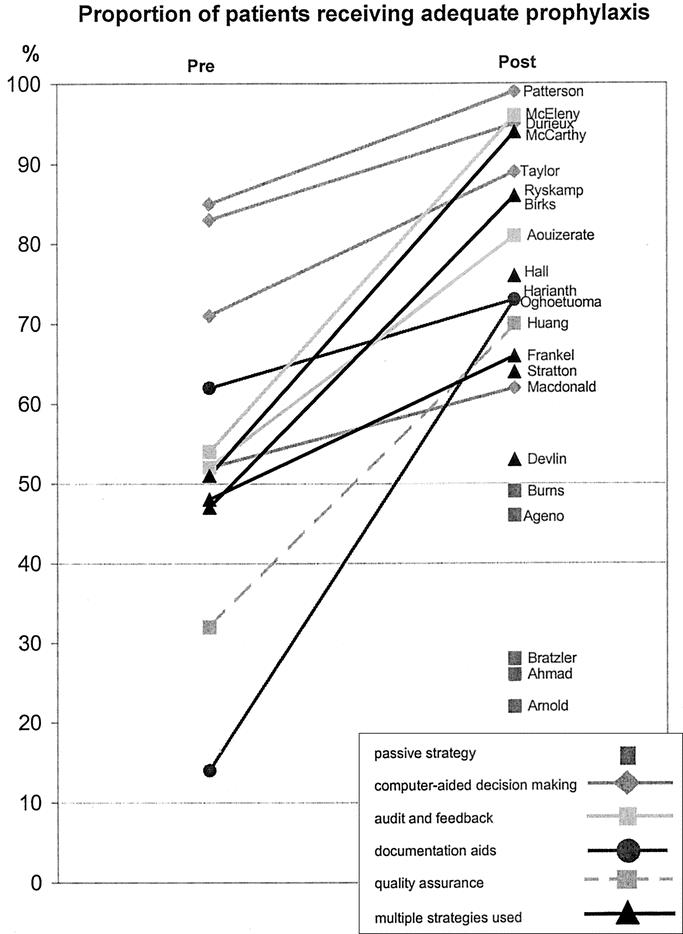
Results: Thirty studies were included. The quality of the available evidence was average with the majority of studies being uncontrolled before and after design and thus limited by the historical nature of much of the available data. Adherence to guidelines and the provision of adequate prophylaxis were poor in studies which relied on passive dissemination of guidelines. In general, the use of multiple strategies was more effective than a single strategy used in isolation. The most effective strategies incorporated a system for reminding clinicians to assess patients for VTE risk, either electronic decision-support systems or paper-based reminders, and used audit and feedback to facilitate the iterative refinement of the intervention. There were no studies adequately powered to demonstrate a reduction in rates of VTE. Insufficient evidence was available to make useful comparisons of strategies in terms of costs and resource utilization.
Conclusions: Passive dissemination of guidelines is unlikely to improve VTE prophylaxis practice. A number of active strategies used together, which incorporate some method for reminding clinicians to assess patients for DVT risk and assisting the selection of appropriate prophylaxis, are likely to result in the achievement of optimal outcomes.
Figures
References
-
- Nicolaides A, Breddin H, Fareed J, et al. Prevention of venous thromboembolism: international consensus statement. J Vasc Bras. 2002;1:133–170. - PubMed
-
- Scottish Intercollegiate Guidelines Network. Prophylaxis of venous thromboembolism: a National Clinical Guideline. Available at: http://www.guideline.gov/summary/summary.aspx?ss=15&doc_id=3485&nbr=2711.... Accessed May 2003.
-
- American College of Chest Physicians. The sixth (2000) ACCP guidelines for antithrombotic therapy for prevention and treatment of thrombosis. Chest. 2002;119. - PubMed
-
- Clagett G, Anderson F, Levine M, et al. Prevention of venous thromboembolism. Chest. 1992;102(suppl 4):391S–407S - PubMed
-
- Clagett G, Anderson F, Heit J, et al. Prevention of venous thromboembolism. Chest. 1995;108(suppl 4):312S–334S. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
