

A prospective randomized study to test the transfer of basic psychomotor skills from virtual reality to physical reality in a comparable training setting
- PMID: 15729066
- PMCID: PMC1356982
- DOI: 10.1097/01.sla.0000154552.89886.91
A prospective randomized study to test the transfer of basic psychomotor skills from virtual reality to physical reality in a comparable training setting
Abstract
Objective: To test whether basic skills acquired on a virtual endoscopic surgery simulator are transferable from virtual reality to physical reality in a comparable training setting.
Summary background data: For surgical training in laparoscopic surgery, new training methods have to be developed that allow surgeons to first practice in a simulated setting before operating on real patients. A virtual endoscopic surgery trainer (VEST) has been developed within the framework of a joint project. Because of principal limitations of simulation techniques, it is essential to know whether training with this simulator is comparable to conventional training.
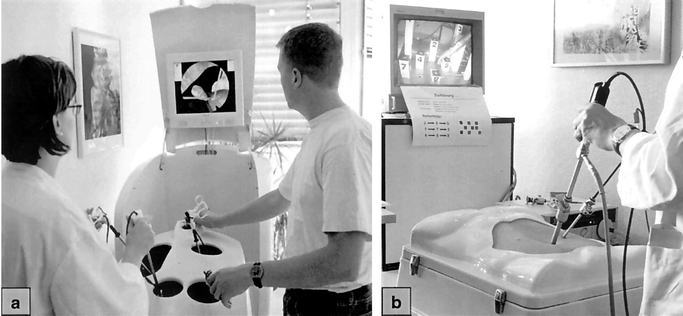
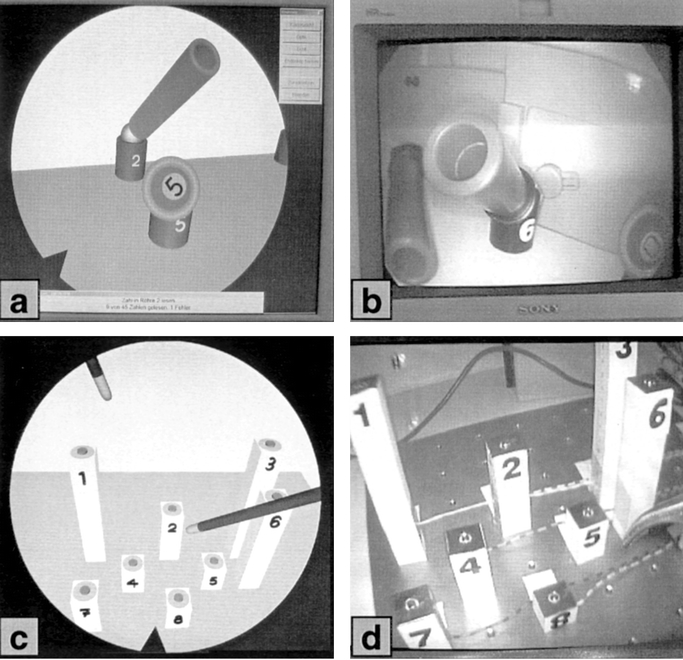
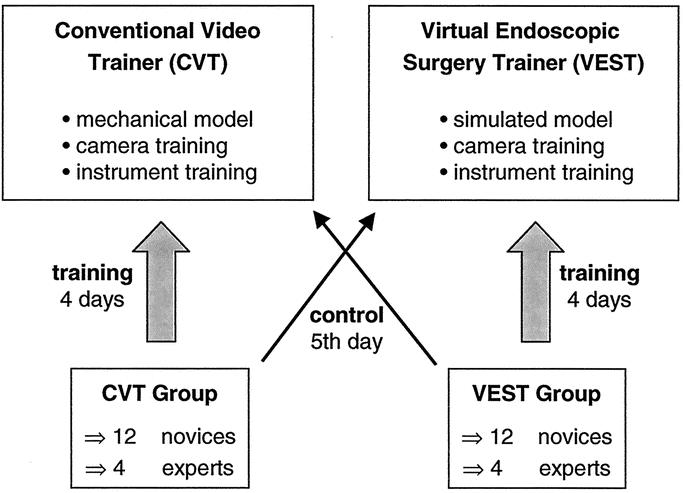
Methods: Devices used were the VEST system and a conventional video trainer (CVT). Two basic training tasks were constructed identically (a) as virtual tasks and (b) as mechanical models for the CVT. Test persons were divided into 2 groups each consisting of 12 novices and 4 experts. Each group carried out a defined training program over the course of 4 consecutive days on the VEST or the CVT, respectively. To test the transfer of skills, the groups switched devices on the 5th day. The main parameter was task completion time.
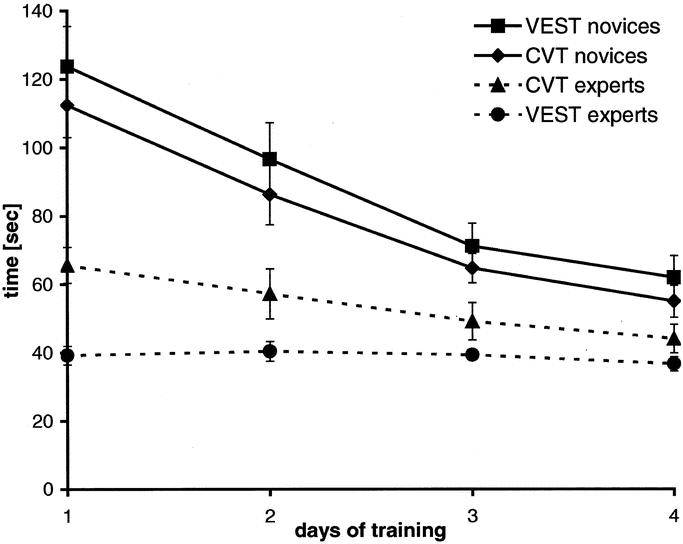
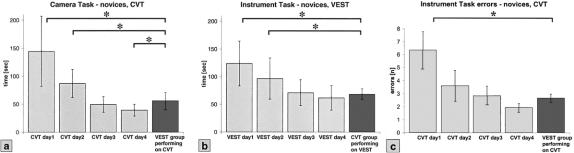
Results: The novices in both groups showed similar learning curves. The mean task completion times decreased significantly over the 4 training days of the study. The task completion times for the control task on Day 5 were significantly lower than on Days 1 and 2. The experts' task completion times were much lower than those of the novices.
Conclusions: This study showed that training with a computer simulator, just as with the CVT, resulted in a reproducible training effect. The control task showed that skills learned in virtual reality are transferable to the physical reality of a CVT. The fact that the experts showed little improvement demonstrates that the simulation trains surgeons in basic laparoscopic skills learned in years of practice.
Figures
References
-
- Richardson MC, Bell G, Fullarton GM. Incidence and nature of bile duct injuries following laparoscopic cholecystectomy: an audit of 5913 cases. West of Scotland Laparoscopic Cholecystectomy Audit Group. Br J Surg. 1996;83:1356–1360. - PubMed
-
- Dent TL. The impact of laparoscopic surgery on health care delivery. The learning curve: skills and privileges. J Laparoendosc Surg. 1993;3:247–249. - PubMed
-
- Hawasli A, Lloyd LR. Laparoscopic cholecystectomy. The learning curve: report of 50 patients. Am Surg. 1991;57:542–544. - PubMed
-
- Moore MJ, Bennett CL. The learning curve for laparoscopic cholecystectomy. The Southern Surgeons Club. Am J Surg. 1995;170:55–59. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
