

Sphincter-saving resection for all rectal carcinomas: the end of the 2-cm distal rule
- PMID: 15729069
- PMCID: PMC1356985
- DOI: 10.1097/01.sla.0000154551.06768.e1
Sphincter-saving resection for all rectal carcinomas: the end of the 2-cm distal rule
Abstract
Objective: To assess oncologic outcome of patients treated by conservative radical surgery for tumors below 5 cm from the anal verge.
Summary background data: Standard surgical treatment of low rectal cancer below 5 cm from the anal verge is abdominoperineal resection.
Methods: From 1990 to 2003, patients with a nonfixed rectal carcinoma at 4.5 cm or less from the anal verge and without external sphincter infiltration underwent conservative surgery. Surgery included total mesorectal excision with intersphincteric resection, that is, removal of the internal sphincter, to achieve adequate distal margin. Patients with T3 disease or internal sphincter infiltration received preoperative radiotherapy.
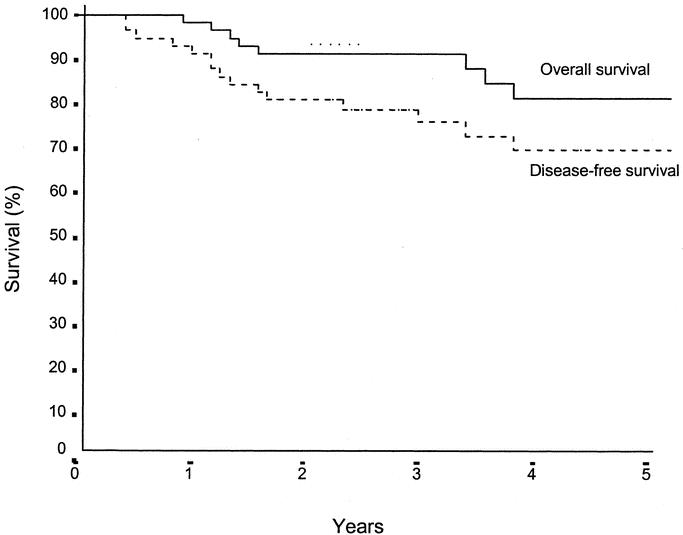
Results: Ninety-two patients with a tumor at 3 (range 1.5-4.5) cm from the anal verge underwent conservative surgery. There was no mortality and morbidity was 27%. The rate of complete microscopic resection (R0) was 89%, with 98% negative distal margin and 89% negative circumferential margin. In 58 patients with a follow-up of more than 24 months, the rate of local recurrence was 2% and the 5-year overall and disease-free survival were 81% and 70%, respectively.
Conclusions: The technique of intersphincteric resection permits us to achieve conservative surgery in patients with a tumor close to or in the anal canal without compromising local control and survival. Tumor distance from the anal verge is no longer a limit for sphincter-saving resection.
Figures

Comment in
-
Sphincter saving resection: end of the 2 cm rule?Ann Surg. 2005 Dec;242(6):903; author reply 903-4. doi: 10.1097/01.sla.0000190050.16795.50. Ann Surg. 2005. PMID: 16327504 Free PMC article. No abstract available.
References
-
- Heald RJ, Moran BJ, Ryall RD, et al. Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978–1997. Arch Surg. 1998;133:894–899. - PubMed
-
- Goligher JC, Dukes CE, Bussey HJR. Local recurrence after sphincter saving excisions for carcinoma of the rectum and rectosigmoid. Br J Surg. 1951;39:199. - PubMed
-
- Localio SA, Eng K. Sphincter-saving operations for cancer of the rectum. N Engl J Med. 1979;300:1028–1030. - PubMed
-
- Tytherleigh MG, Mortensen NJMcC. Options for sphincter preservation in surgery for low rectal cancer. Br J Surg. 2003;90:922–933. - PubMed
-
- Williams NS, Dixon MF, Johnston D. Reappraisal of the 5 centimetre rule of distal excision for carcinoma of the rectum: a study of distal intramural spread and of patients survival. Br J Surg. 1983;70:150–154. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
