

Improved outcome in HLA-identical sibling hematopoietic stem-cell transplantation for acute myelogenous leukemia predicted by KIR and HLA genotypes
- PMID: 15731175
- PMCID: PMC1894998
- DOI: 10.1182/blood-2004-12-4825
Improved outcome in HLA-identical sibling hematopoietic stem-cell transplantation for acute myelogenous leukemia predicted by KIR and HLA genotypes
Abstract
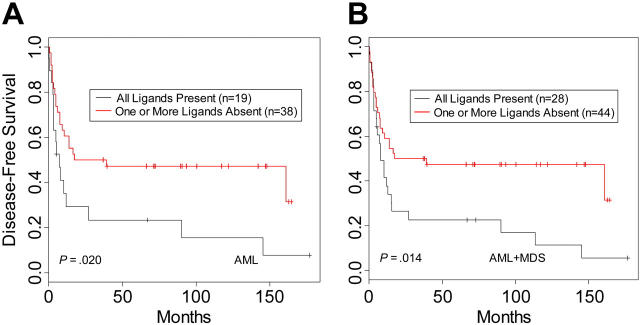
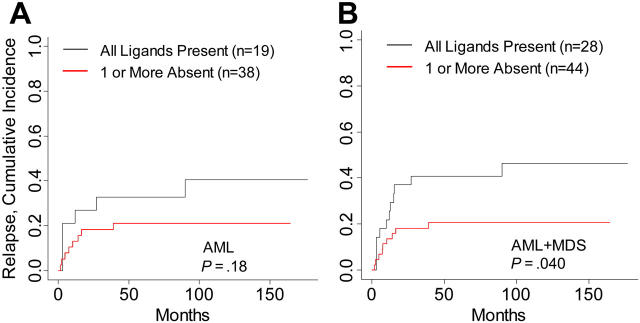
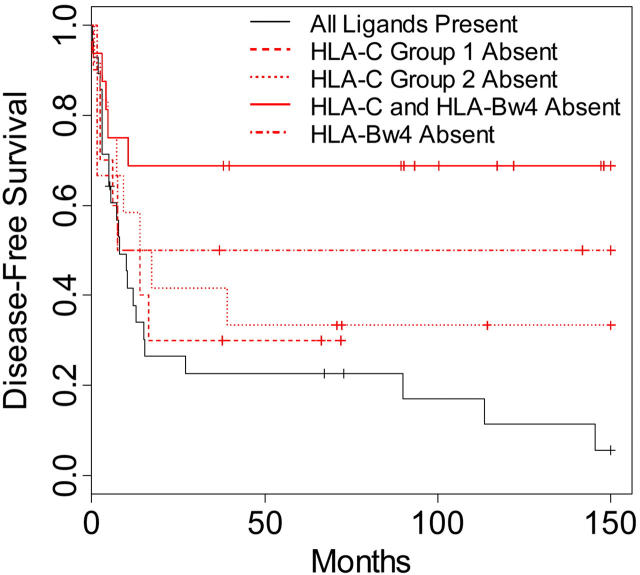
Inhibitory killer immunoglobulin (Ig)-like receptors (KIRs) recognize HLA-C and -B epitopes on target cells, thereby regulating natural killer (NK) cell activity. In 178 patients receiving T-cell-depleted HLA-identical sibling transplants for acute myelogenous leukemia (AML), chronic myelogenous leukemia (CML), acute lymphoblastic leukemia (ALL), or myelodysplastic syndrome (MDS), analysis of donor KIR genotype with HLA genotype demonstrated that 62.9% of the patients lacked an HLA ligand for donor-inhibitory KIR. Lack of HLA ligand for donor-inhibitory KIR (missing KIR ligand) had no effect on disease-free survival (DFS), overall survival (OS), or relapse in patients receiving transplants for CML and ALL. In patients with AML and MDS, however, there was a significant missing KIR ligand effect on DFS (P = .014; hazard ratio [HR], 0.53; 95% confidence interval [95% CI], 0.28-0.88) and OS (P = .03; HR, 0.53; 95% CI, 0.3-0.93). Incidence of relapse was also lower in patients with AML and MDS who lacked the HLA ligand for donor-inhibitory KIR (P = .04; HR, 0.41; 95% CI, 0.18-0.97). AML and MDS patients lacking 2 HLA ligands for donor-inhibitory KIR had the highest DFS (P = .002) and OS (P = .003). There was no significant contribution of donor-activating KIR to transplantation outcome in these patients. These data indicate that the absence of class I ligand in the recipient for donor-inhibitory KIR can be a prognostic factor for transplantation outcome in HLA-identical sibling transplantation and that the lack of HLA-C or -B ligands for donor-inhibitory KIR can contribute to improved outcomes for patients with AML and MDS.
Figures
References
-
- Ruggeri L, Capanni M, Casucci M, et al. Role of natural killer cell alloreactivity in HLA-mismatched hematopoietic stem cell transplantation. Blood. 1999;94: 333-339. - PubMed
-
- Ruggeri L, Capanni M, Urbani E, et al. Effectiveness of donor natural killer cell alloreactivity in mismatched hematopoietic transplants. Science. 2002;295: 2097-2100. - PubMed
-
- Biron CA, Nguyen KB, Pien GC, Cousens LP, Salazar-Mather TP. Natural killer cells in antiviral defense: function and regulation by innate cytokines. Annu Rev Immunol. 1999;17: 189-220. - PubMed
-
- Inoue H, Yasuda Y, Hattori K, et al. The kinetics of immune reconstitution after cord blood transplantation and selected CD34+ stem cell transplantation in children: comparison with bone marrow transplantation. Int J Hematol. 2003;77: 399-407. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
