

Cardiac stem cells delivered intravascularly traverse the vessel barrier, regenerate infarcted myocardium, and improve cardiac function
- PMID: 15734798
- PMCID: PMC553298
- DOI: 10.1073/pnas.0405957102
Cardiac stem cells delivered intravascularly traverse the vessel barrier, regenerate infarcted myocardium, and improve cardiac function
Abstract
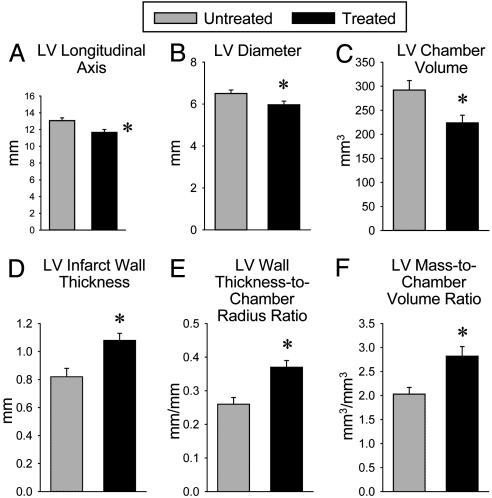
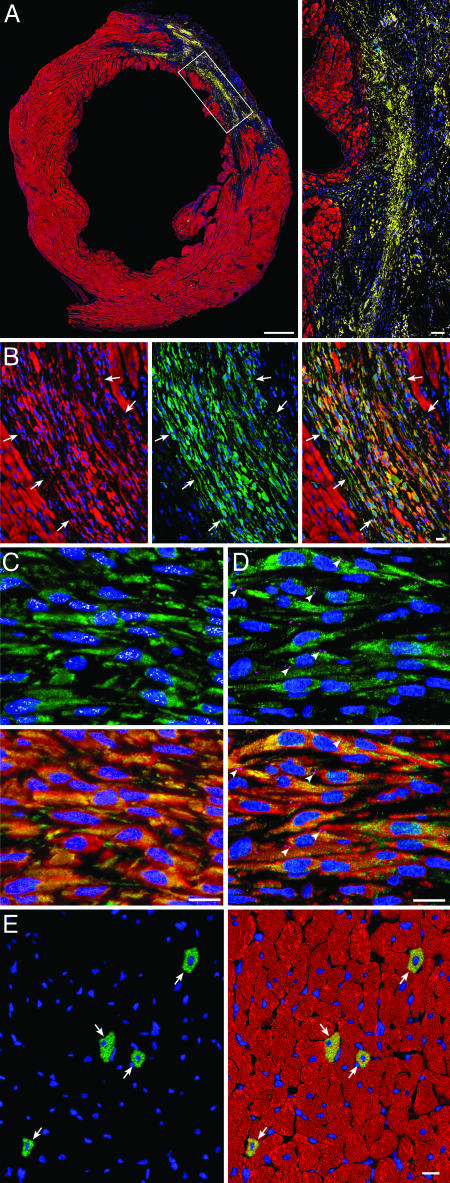
The ability of cardiac stem cells (CSCs) to promote myocardial repair under clinically relevant conditions (i.e., when delivered intravascularly after reperfusion) is unknown. Thus, rats were subjected to a 90-min coronary occlusion; at 4 h after reperfusion, CSCs were delivered to the coronary arteries via a catheter positioned into the aortic root. Echocardiographic analysis showed that injection of CSCs attenuated the increase in left ventricular (LV) end-diastolic dimensions and impairment in LV systolic performance at 5 weeks after myocardial infarction. Pathologic analysis showed that treated hearts exhibited a smaller increase in LV chamber diameter and volume and a higher wall thickness-to-chamber radius ratio and LV mass-to-chamber volume ratio. CSCs induced myocardial regeneration, decreasing infarct size by 29%. A diploid DNA content and only two chromosomes 12 were found in new cardiomyocytes, indicating that cell fusion did not contribute to tissue reconstitution. In conclusion, intravascular injection of CSCs after reperfusion limits infarct size, attenuates LV remodeling, and ameliorates LV function. This study demonstrates that CSCs are effective when delivered in a clinically relevant manner, a clear prerequisite for clinical translation, and that these beneficial effects are independent of cell fusion. The results establish CSCs as candidates for cardiac regeneration and support an approach in which the heart's own stem cells could be collected, expanded, and stored for subsequent therapeutic repair.
Figures



References
-
- Rosenthal, N. (2003) N. Engl. J. Med. 349, 267-274. - PubMed
-
- Strauer, B. E., Brehm, M., Zeus, T., Kostering, M., Hernandez, A., Sorg, R. V., Kogler, G. & Wernet, P. (2002) Circulation 106, 1913-1918. - PubMed
-
- Britten, M. B., Abolmaali, N. D., Assmus, B., Lehmann, R., Honold, J., Schmitt, J., Vogl, T. J., Martin, H., Schachinger, V., Dimmeler, S., et al. (2003) Circulation 108, 2212-2218. - PubMed
-
- Perin, E. C., Dohmann, H. F., Borojevic, R., Silva, S. A., Sousa, A. L., Mesquita, C. T., Rossi, M. I., Carvalho, A. C., Dutra, H. S., Dohmann, H. J., et al. (2003) Circulation 107, 2294-2302. - PubMed
-
- Stamm, C., Westphal, B., Kleine, H. D., Petzsch, M., Kittner, C., Klinge, H., Schumichen, C., Nienaber, C. A., Freund, M. & Steinhoff, G. (2003) Lancet 361, 45-46. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 AG017042/AG/NIA NIH HHS/United States
- R01 HL076794/HL/NHLBI NIH HHS/United States
- AG 023071/AG/NIA NIH HHS/United States
- R01 HL055757/HL/NHLBI NIH HHS/United States
- R01 HL038132/HL/NHLBI NIH HHS/United States
- HL 65577/HL/NHLBI NIH HHS/United States
- HL 72410/HL/NHLBI NIH HHS/United States
- HL 68088/HL/NHLBI NIH HHS/United States
- R01 HL070897/HL/NHLBI NIH HHS/United States
- HL 39902/HL/NHLBI NIH HHS/United States
- HL 66923/HL/NHLBI NIH HHS/United States
- R01 HL072410/HL/NHLBI NIH HHS/United States
- HL 38132/HL/NHLBI NIH HHS/United States
- R01 HL 55757/HL/NHLBI NIH HHS/United States
- HL 70897/HL/NHLBI NIH HHS/United States
- HL 76794/HL/NHLBI NIH HHS/United States
- AG 15756/AG/NIA NIH HHS/United States
- R01 HL039902/HL/NHLBI NIH HHS/United States
- AG 17042/AG/NIA NIH HHS/United States
- R01 HL065577/HL/NHLBI NIH HHS/United States
- P01 AG023071/AG/NIA NIH HHS/United States
- HL 65573/HL/NHLBI NIH HHS/United States
- R01 HL065573/HL/NHLBI NIH HHS/United States
- R01 HL068088/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
