

Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance, and hyperglycemia by moderate weight reduction in patients with type 2 diabetes
- PMID: 15734833
- PMCID: PMC2995496
- DOI: 10.2337/diabetes.54.3.603
Reversal of nonalcoholic hepatic steatosis, hepatic insulin resistance, and hyperglycemia by moderate weight reduction in patients with type 2 diabetes
Abstract
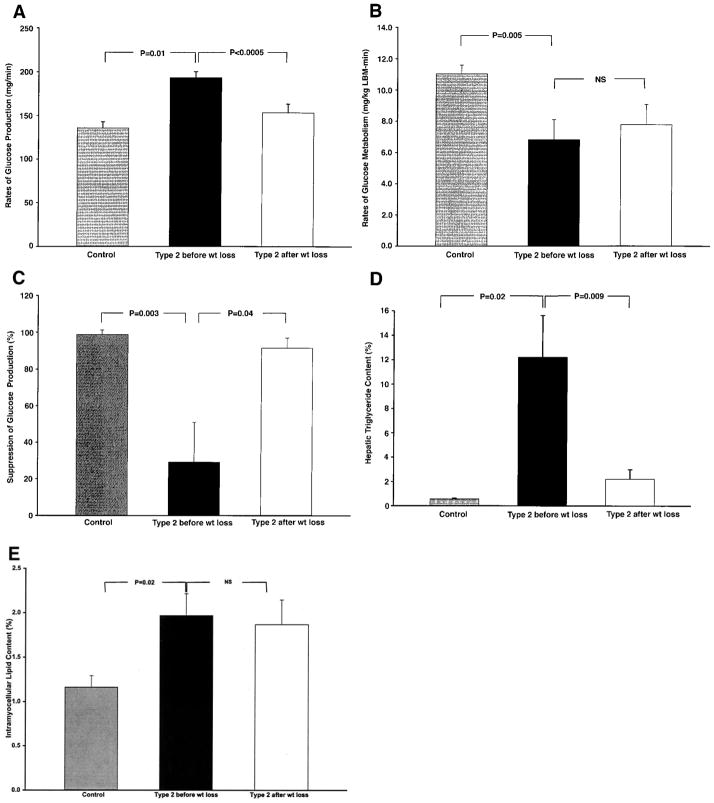
To examine the mechanism by which moderate weight reduction improves basal and insulin-stimulated rates of glucose metabolism in patients with type 2 diabetes, we used (1)H magnetic resonance spectroscopy to assess intrahepatic lipid (IHL) and intramyocellular lipid (IMCL) content in conjunction with hyperinsulinemic-euglycemic clamps using [6,6-(2)H(2)]glucose to assess rates of glucose production and insulin-stimulated peripheral glucose uptake. Eight obese patients with type 2 diabetes were studied before and after weight stabilization on a moderately hypocaloric very-low-fat diet (3%). The diabetic patients were markedly insulin resistant in both liver and muscle compared with the lean control subjects. These changes were associated with marked increases in IHL (12.2 +/- 3.4 vs. 0.6 +/- 0.1%; P = 0.02) and IMCL (2.0 +/- 0.3 vs. 1.2 +/- 0.1%; P = 0.02) compared with the control subjects. A weight loss of only approximately 8 kg resulted in normalization of fasting plasma glucose concentrations (8.8 +/- 0.5 vs. 6.4 +/- 0.3 mmol/l; P < 0.0005), rates of basal glucose production (193 +/- 7 vs. 153 +/- 10 mg/min; P < 0.0005), and the percentage suppression of hepatic glucose production during the clamp (29 +/- 22 vs. 99 +/- 3%; P = 0.003). These improvements in basal and insulin-stimulated hepatic glucose metabolism were associated with an 81 +/- 4% reduction in IHL (P = 0.0009) but no significant change in insulin-stimulated peripheral glucose uptake or IMCL (2.0 +/- 0.3 vs. 1.9 +/- 0.3%; P = 0.21). In conclusion, these data support the hypothesis that moderate weight loss normalizes fasting hyperglycemia in patients with poorly controlled type 2 diabetes by mobilizing a relatively small pool of IHL, which reverses hepatic insulin resistance and normalizes rates of basal glucose production, independent of any changes in insulin-stimulated peripheral glucose metabolism.
Figures
References
-
- Henry RR, Scheaffer L, Olefsky JM. Glycemic effects of intensive caloric restriction and isocaloric refeeding in noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1985;61:917–925. - PubMed
-
- Petersen KF, Price T, Cline GW, Rothman DL, Shulman GI. Contribution of net hepatic glycogenolysis to glucose production during the early postprandial period. Am J Physiol. 1996;270:E186–E191. - PubMed
-
- Mayerson AB, Hundal RS, Dufour S, Lebon V, Befroy D, Cline GW, Enocksson S, Inzucchi SE, Shulman GI, Petersen KF. The effects of rosiglitazone on insulin sensitivity, lipolysis, and hepatic and skeletal muscle triglyceride content in patients with type 2 diabetes. Diabetes. 2002;51:797–802. - PMC - PubMed
-
- Lusk G. Animal calorimetry: analysis of the oxidation of mixtures of carbohydrates and fat: a correction. J Biol Chem. 1924;59:41–42.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
