

Ultrarapid Ki-67 immunostaining in frozen section interpretation of gliomas
- PMID: 15735157
- PMCID: PMC1770597
- DOI: 10.1136/jcp.2004.018606
Ultrarapid Ki-67 immunostaining in frozen section interpretation of gliomas
Abstract
Background: Astrocytic tumours, the most common gliomas, are often classified intraoperatively using standard morphological staining. The final diagnosis and grading of gliomas on paraffin wax sections is often assisted by Ki-67 immunohistochemistry, but standard immunostaining protocols take too long to be used intraoperatively.
Aims: To investigate a new rapid Ki-67 immunohistochemical test for its use in an intraoperative setting.
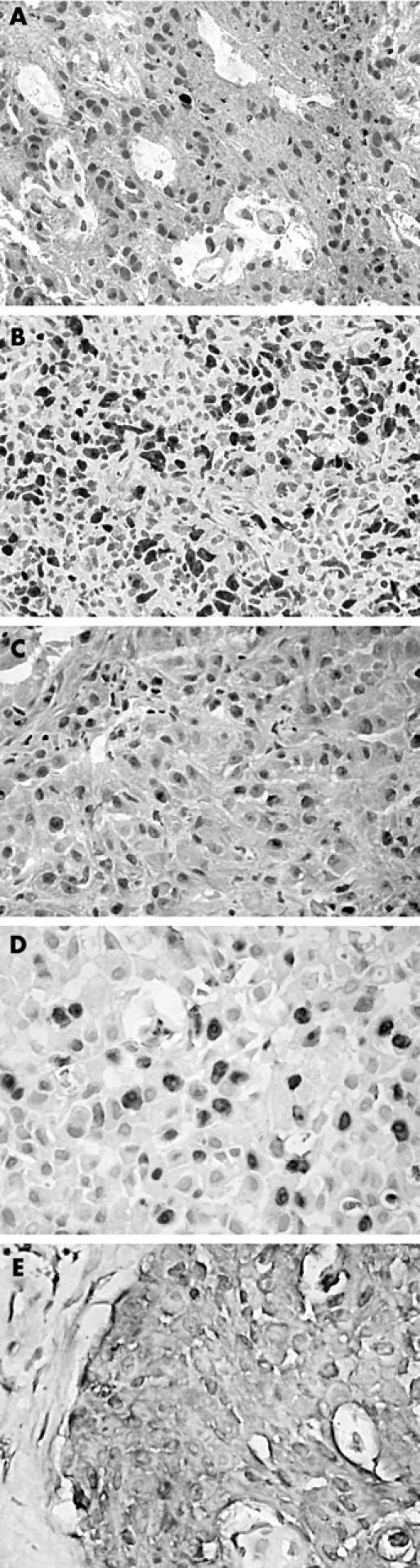
Methods: The new Ki-67 immunostaining (Ultrarapid-Ki67) method on frozen sections can be carried out in 10 minutes. Thirty four pilocytic and diffuse astrocytomas were immunostained by rapid Ki-67 and results were compared with corresponding MIB-1 staining, histological grading, and prognosis.
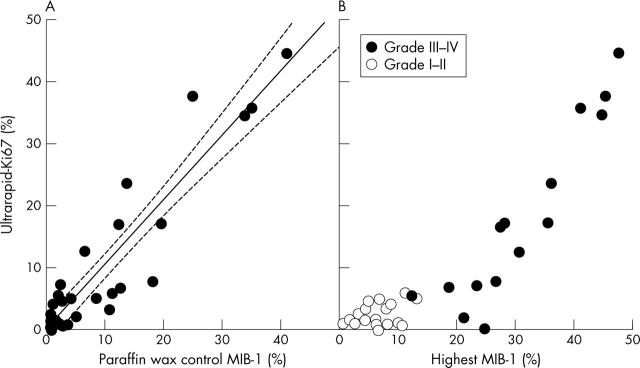
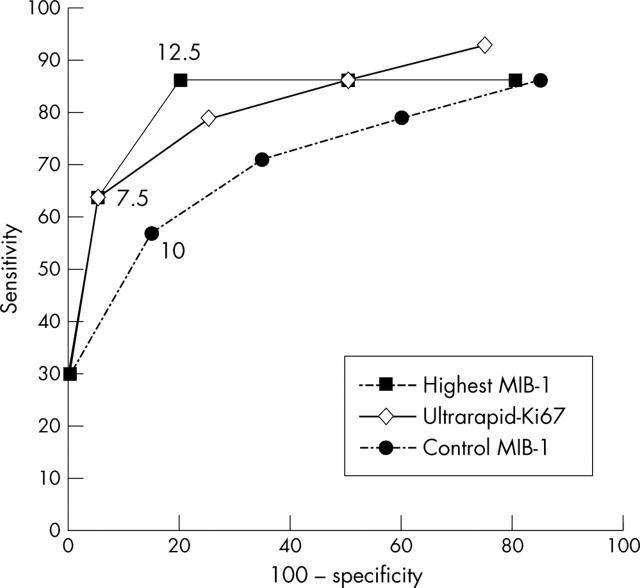
Results: The staining protocol was practical to perform and the results were morphologically and quantitatively indistinguishable from those after immunostaining with MIB-1, an antibody recognising Ki-67 in paraffin wax embedded tissue. A comparison of Ultrarapid-Ki67 and MIB-1 immunostaining of paraffin wax sections showed almost identical quantitative correlation in astrocytic gliomas (r = 0.916; p<0.001). The Ultrarapid-Ki67 indices (percentage of positive cells) of low grade (I/II) astrocytomas ranged from 0% to 6.1%, whereas those of representative high grade (III/IV) tumours were significantly higher (range, 5.6-45%; p<0.001). The best prognostic cutoff point for Ultrarapid-Ki67 was 7.5%, which divided diffuse grade II-IV astrocytomas into significantly differing subsets (p = 0.0008).
Conclusion: Ultrarapid-Ki67 immunostaining is a useful adjunct to morphological diagnosis and grading of astrocytic tumours, and as a fast test (approximately 10 minutes for staining plus three to four minutes for scoring), it could be used in routine intraoperative diagnosis of gliomas and other neoplastic diseases.
Figures
References
-
- Shah A, Muzumdar G, Chitale A, et al. Squash preparation and frozen section in intraoperative diagnosis of central nervous system tumors. Acta Cytol 1998;42:1149–54. - PubMed
-
- Kleihues P, Cavenee WK, eds. Pathology and genetics of tumours of the nervous system. WHO classification of tumours. Lyon: IARC Press, 2000.
-
- Giannini C, Scheithauer PW, Burger PC, et al. Cellular proliferation in pilocytic and diffuse astrocytomas. J Neuropathol Exp Neurol 1999;58:46–53. - PubMed
-
- Burger PC, Shibata T, Kleihues P. The use of monoclonal antibody Ki-67 in the identification of proliferating cells: application to surgical neuropathology. Am J Surg Pathol 1986;10:611–17. - PubMed
-
- Sallinen P, Haapasalo H, Visakorpi T, et al. Relation of Ki-67 (MIB-1), PCNA and S-phase fraction with patient survival in formalin-fixed, paraffin-embedded astrocytoma material. J Pathol 1994;174:275–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical