

Youth type 2 diabetes: insulin resistance, beta-cell failure, or both?
- PMID: 15735201
- PMCID: PMC3428068
- DOI: 10.2337/diacare.28.3.638
Youth type 2 diabetes: insulin resistance, beta-cell failure, or both?
Abstract
Objective: This study evaluates insulin sensitivity, pancreatic beta-cell function (BCF), and the balance between the two in youth with type 2 diabetes and assesses the relationship of diabetes duration and HbA(1c) to insulin sensitivity and BCF.
Research design and methods: The subjects were 14 adolescents with type 2 diabetes and 20 obese control subjects of comparable age, BMI, body composition, and puberty. Insulin sensitivity was evaluated with a 3-h hyperinsulinemic (80 mU . m(-2) . min(-1)) euglycemic clamp. First-phase insulin secretion (FPIS) and second-phase insulin secretion (SPIS) were evaluated with a 2-h hyperglycemic (12.5 mmol/l) clamp. Fasting glucose rate of appearance was determined with the use of [6,6-(2)H(2)]glucose.
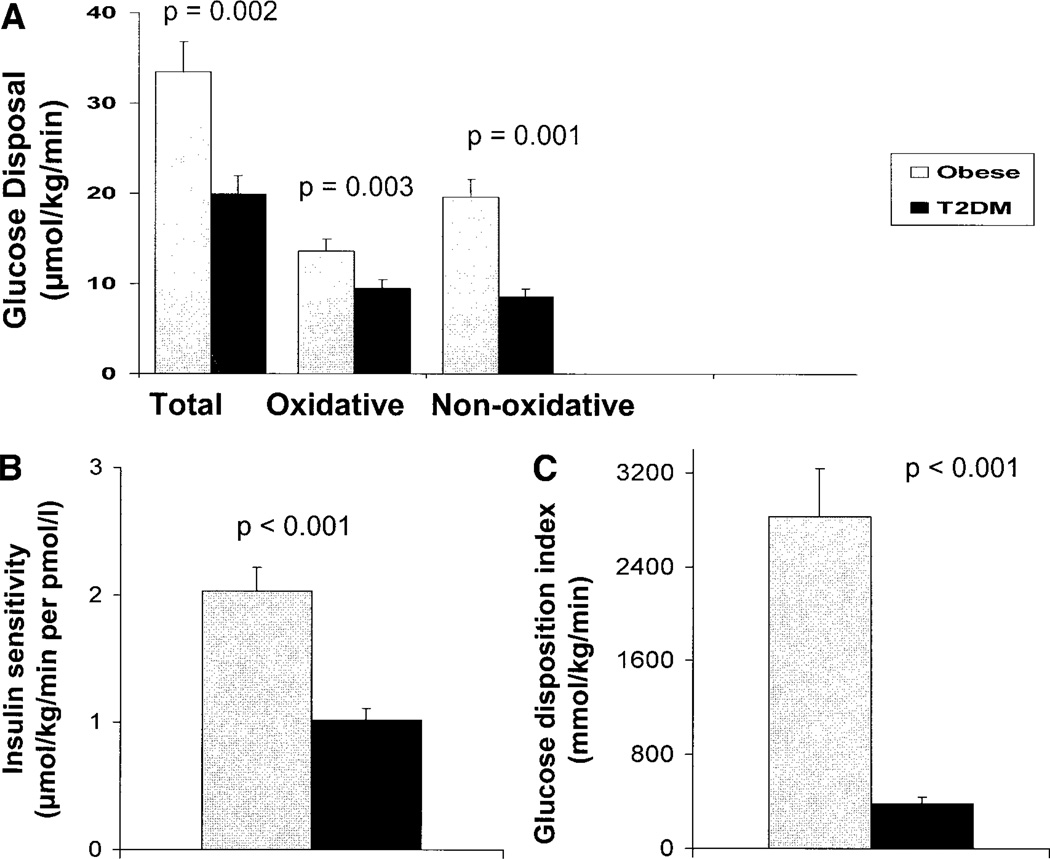
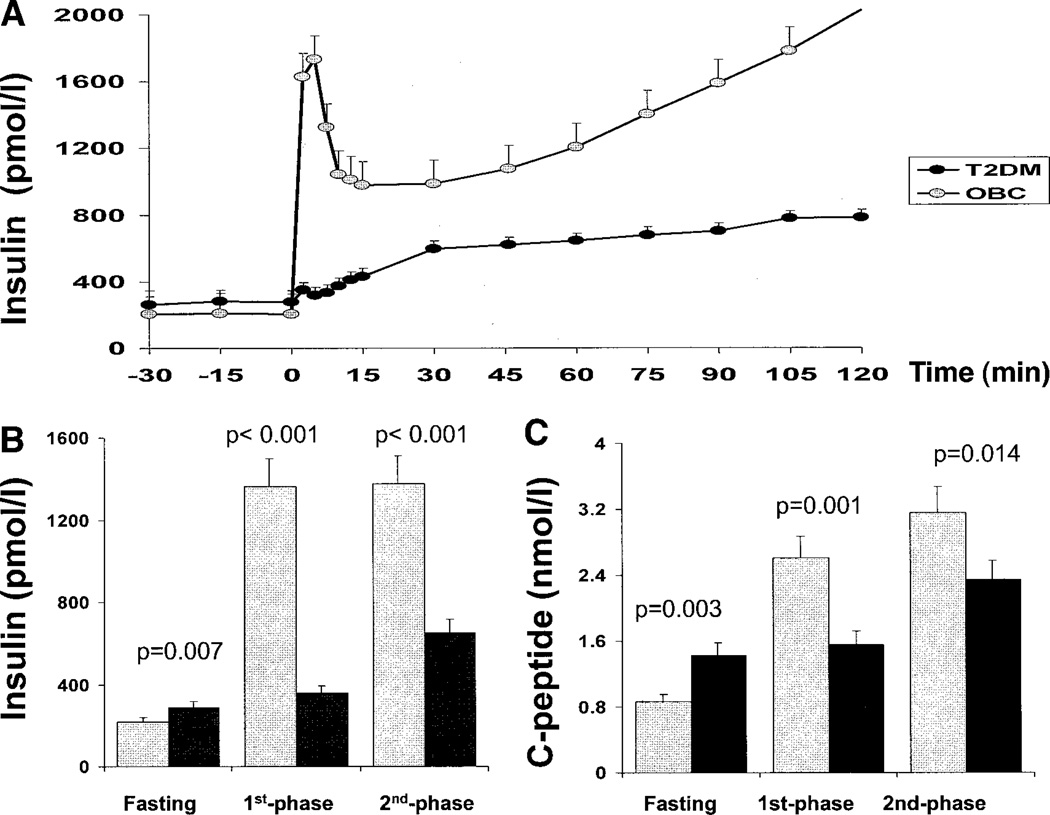
Results: Fasting glucose rate of appearance was higher in type 2 diabetic patients than in obese control subjects (16.5 +/- 1.1 vs. 12.3 +/- 0.5 micromol . kg(-1) . min(-1); P = 0.002). Insulin sensitivity was lower in type 2 diabetic patients than in obese control subjects (1.0 +/- 0.1 vs. 2.0 +/- 0.2 micromol . kg(-1) . min(-1) per pmol/l; P = 0.001). Fasting insulin was higher in type 2 diabetic patients than in obese control subjects (289.8 +/- 24.6 vs. 220.2 +/- 18.0 pmol/l; P = 0.007), and FPIS and SPIS were lower (FPIS: 357.6 +/- 42.0 vs. 1,365.0 +/- 111.0 pmol/l; SPIS: 652.2 +/- 88.8 vs. 1,376.4 +/- 88.8 pmol/l; P < 0.001 for both). The glucose disposition index (GDI = insulin sensitivity x FPIS) was approximately 86% lower in type 2 diabetic patients than in obese control subjects. HbA(1c) correlated with FPIS (r = -0.61, P = 0.025) with no relationship to insulin sensitivity.
Conclusions: Despite the impairment in both insulin sensitivity and BCF in youth with type 2 diabetes, the magnitude of the derangement is greater in BCF than insulin sensitivity when compared with that in obese control subjects. The inverse relationship between BCF and HbA(1c) may either reflect the impact of deteriorating BCF on glycemic control or be a manifestation of a glucotoxic phenomenon on BCF. Future studies in youth type 2 diabetes should target the natural course of beta-cell failure and means of retarding and/or preventing it.
Figures
References
-
- American Diabetes Association. Type 2 diabetes in children and adolescents. Diabetes Care. 2000;23:381–389. - PubMed
-
- Saad MF, Knowler WC, Pettitt DJ, Nelson RG, Charles MA, Bennett PH. A two-step model for development of non-insulindependent diabetes. Am J Med. 1991;90:229–235. - PubMed
-
- Kahn SE. The importance of β-cell failure in the development and progression of type 2 diabetes. J Clin Endocrinol Metab. 2001;86:4047–4058. - PubMed
-
- Banerji MA, Lebovitz HE. Insulin action in black Americans with NIDDM. Diabetes Care. 1992;15:1295–1302. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
