

Thymic output generates a new and diverse TCR repertoire after autologous stem cell transplantation in multiple sclerosis patients
- PMID: 15738052
- PMCID: PMC2212822
- DOI: 10.1084/jem.20041679
Thymic output generates a new and diverse TCR repertoire after autologous stem cell transplantation in multiple sclerosis patients
Abstract
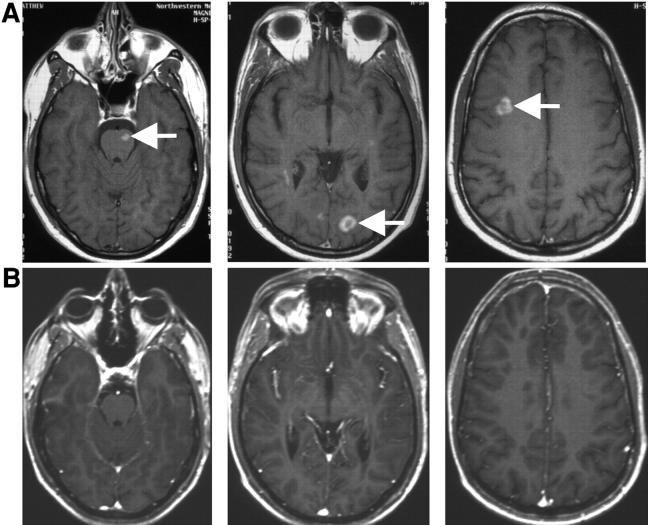
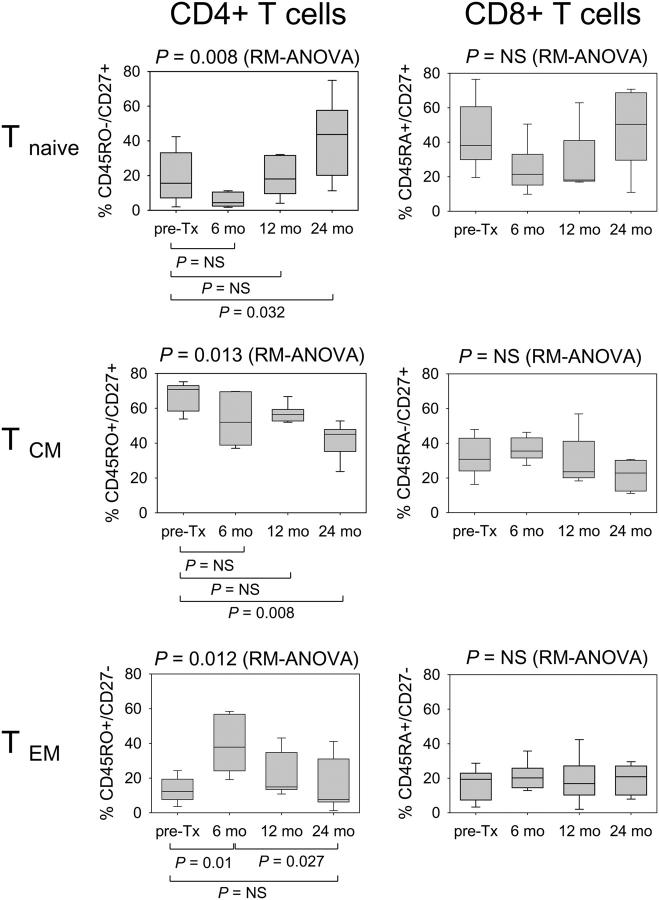
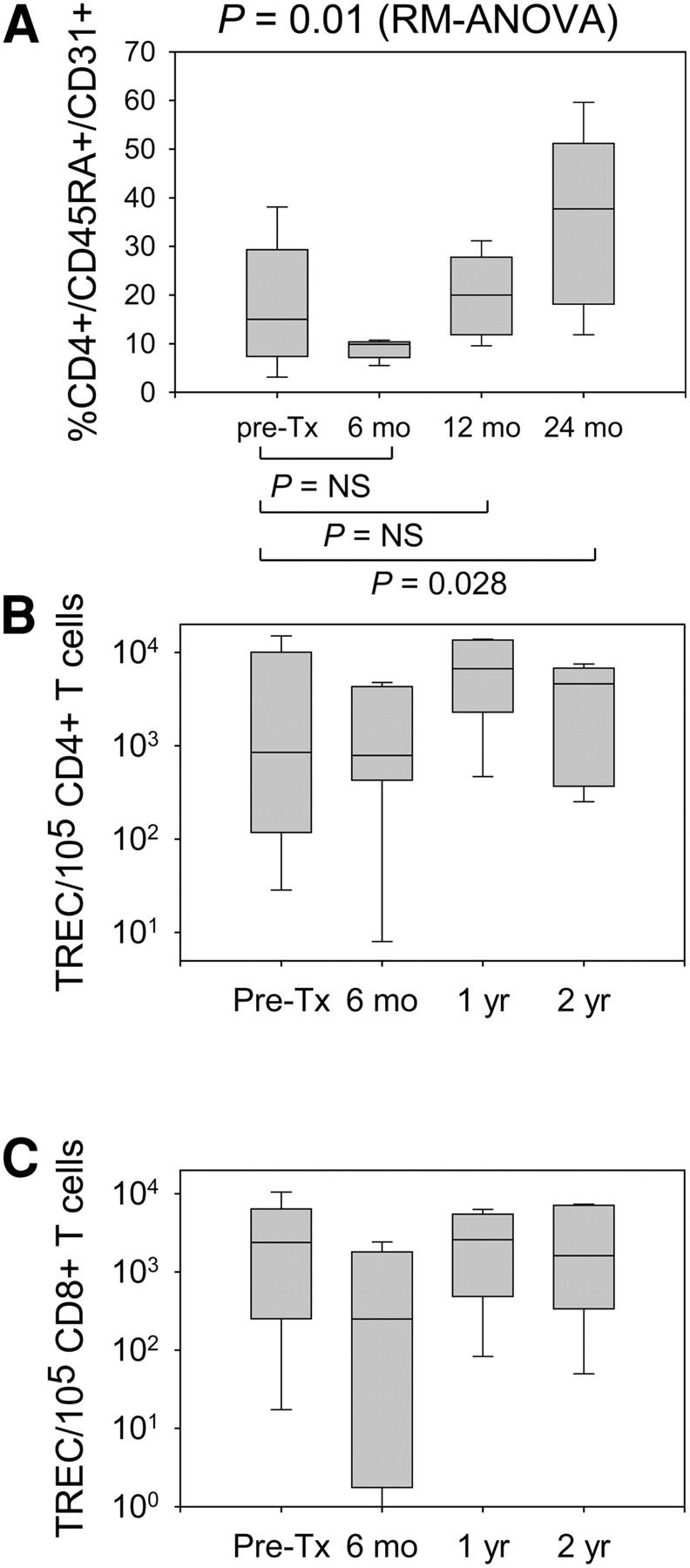
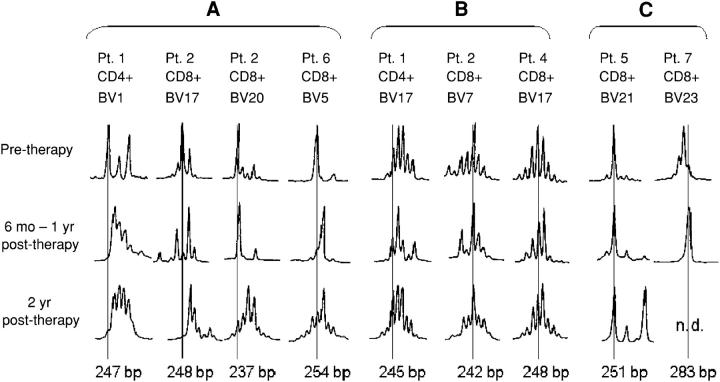
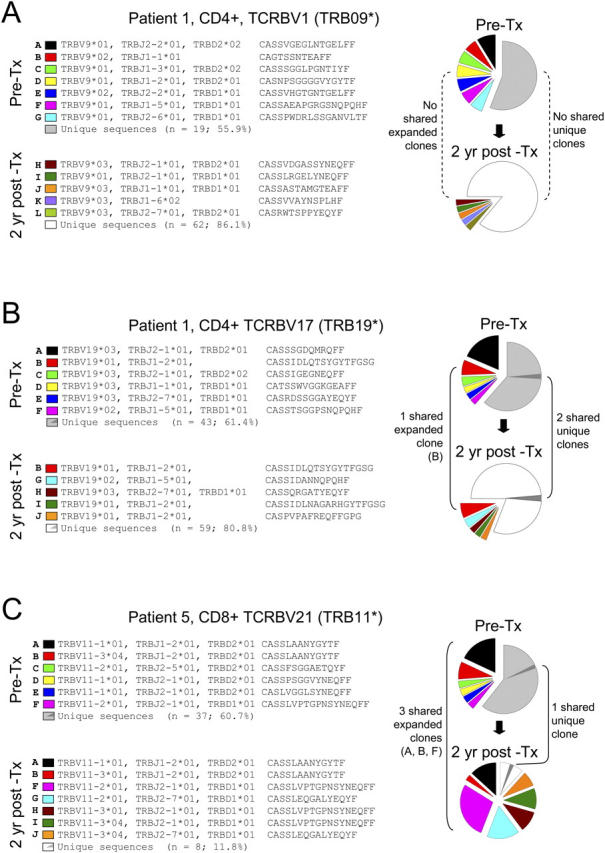
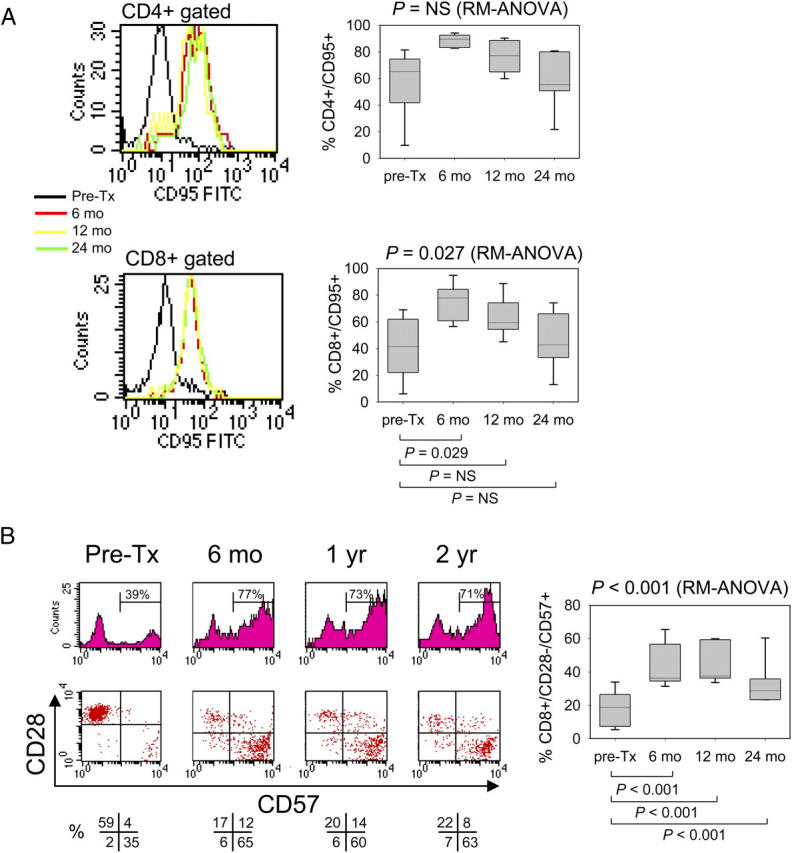
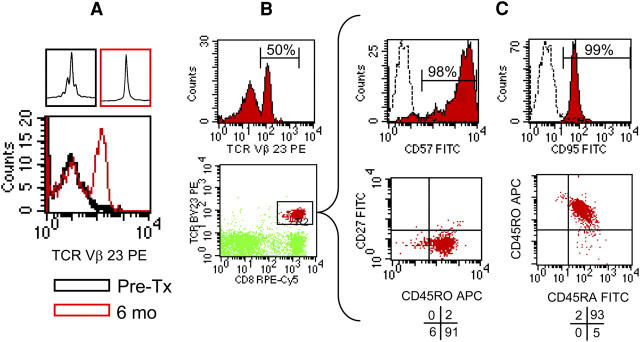
Clinical trials have indicated that autologous hematopoietic stem cell transplantation (HSCT) can persistently suppress inflammatory disease activity in a subset of patients with severe multiple sclerosis (MS), but the mechanism has remained unclear. To understand whether the beneficial effects on the course of disease are mediated by lympho-depletive effects alone or are sustained by a regeneration of the immune repertoire, we examined the long-term immune reconstitution in patients with MS who received HSCT. After numeric recovery of leukocytes, at 2-yr follow-up there was on average a doubling of the frequency of naive CD4(+) T cells at the expense of memory T cells. Phenotypic and T cell receptor excision circle (TREC) analysis confirmed a recent thymic origin of the expanded naive T cell subset. Analysis of the T cell receptor repertoire showed the reconstitution of an overall broader clonal diversity and an extensive renewal of clonal specificities compared with pretherapy. These data are the first to demonstrate that long-term suppression of inflammatory activity in MS patients who received HSCT does not depend on persisting lymphopenia and is associated with profound qualitative immunological changes that demonstrate a de novo regeneration of the T cell compartment.
Figures
References
-
- Muraro, P.A., R. Cassiani Ingoni, and R. Martin. 2003. Hematopoietic stem cell transplantation for multiple sclerosis: current status and future challenges. Curr. Opin. Neurol. 16:299–305. - PubMed
-
- Fassas, A., and V.K. Kimiskidis. 2003. Stem cell transplantation for multiple sclerosis: what is the evidence? Blood Rev. 17:233–240. - PubMed
-
- Burt, R.K., S. Slavin, W.H. Burns, and A.M. Marmont. 2002. Induction of tolerance in autoimmune diseases by hematopoietic stem cell transplantation: getting closer to a cure? Blood. 99:768–784. - PubMed
-
- Fassas, A., A. Anagnostopoulos, A. Kazis, K. Kapinas, I. Sakellari, V. Kimiskidis, and A. Tsompanakou. 1997. Peripheral blood stem cell transplantation in the treatment of progressive multiple sclerosis: first results of a pilot study. Bone Marrow Transplant. 20:631–638. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
