

Verification of inverse planning and treatment delivery for segmental IMRT
- PMID: 15738908
- PMCID: PMC5723460
- DOI: 10.1120/jacmp.v5i2.1975
Verification of inverse planning and treatment delivery for segmental IMRT
Abstract
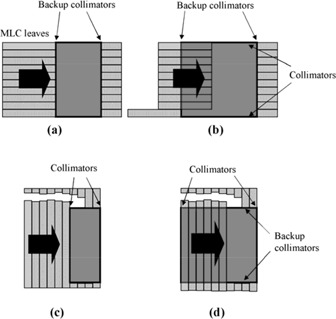
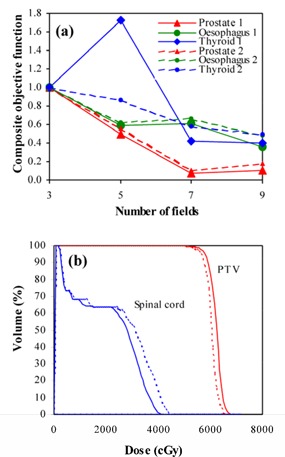
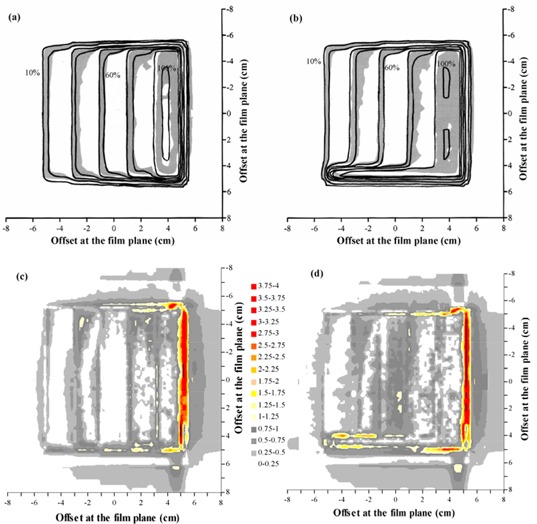
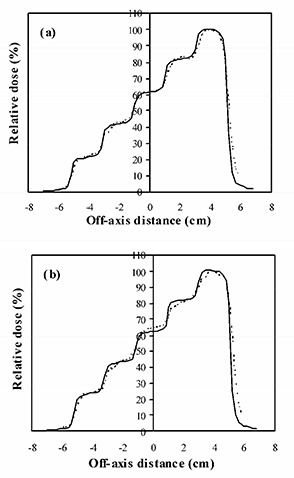
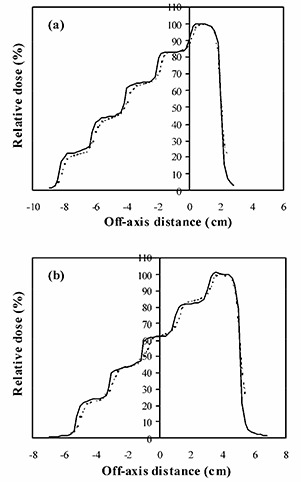
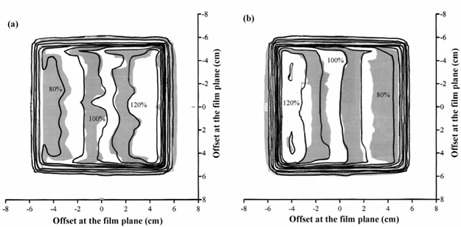
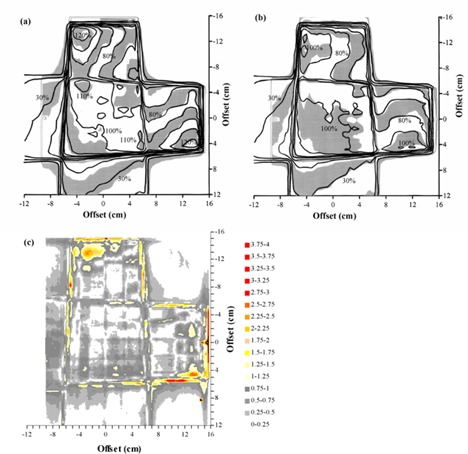
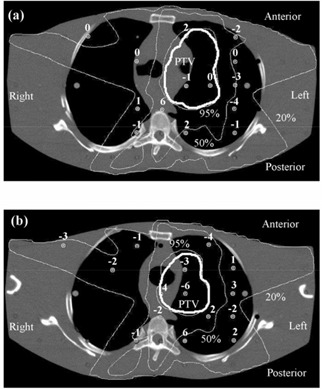
With intensity-modulated radiotherapy (IMRT), it is important that the inverse planning process yields the most appropriate dose distribution for the patient and that the delivered dose then corresponds to the planned dose. This paper presents methods by which the inverse planning and delivery of segmental (step-and-shoot) IMRT can be verified, and gives results for a typical treatment planning system (Pinnacle3 v6.2b, Philips Radiation Oncology Systems, Milpitas, CA). Inverse planning was assessed by observing the reduction in objective function as fields were successively added to three-field prostate, esophagus, and thyroid plans. The ability of the treatment planning system to calculate dose for a segmented field was examined by creating a stepped field with five successively narrowing segments. The complete planning process was then investigated by using two orthogonal IMRT fields to create a homogeneous dose distribution in a cubic water phantom. Finally, a clinical situation was simulated by creating a five-field segmental IMRT plan for a lung target in an anthropomorphic phantom. A conformal plan was also compared for context. Addition of fields to inverse plans generally resulted in a reduction of objective function, indicating consistency of inverse planning solutions. Planned dose for fields with stepped intensity agreed with ionization chamber measurements to within 5%. For orthogonal fields, planned dose distributions agreed well with dose measured using film and agreed with ionization chamber measurements to within 3%. For the anthropomorphic phantom, the standard deviation of difference between planned and measured dose was 4%. Although no consensus has yet been reached on what constitutes an acceptable IMRT plan, these results indicate that step-and-shoot IMRT can be planned and delivered using the system described with comparable accuracy to a standard conformal treatment.
Figures
References
-
- Webb S., Intensity‐modulated radiation therapy, Bristol: Institute of Physics Publishing, 2001.
-
- Xing L., Li J.G., Donaldson S., Le Q.T., and Boyer A.L., Optimization of importance factors in inverse planning, Phys. Med. Biol. 44, 2525–36 (1999). - PubMed
-
- Bedford J.L. and Webb S., Elimination of importance factors for clinically accurate selection of beam orientations, beam weights and wedge angles in conformal radiation therapy, Med. Phys. 30, 1788–804 (2003). - PubMed
-
- Low D.A., Mutic S., Dempsey J.F. et al., Quantitative dosimetric verification of an IMRT planning and delivery system, Radiother. Oncol. 49, 305–16 (1998). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
