

Stereotactic IMRT for prostate cancer: setup accuracy of a new stereotactic body localization system
- PMID: 15738910
- PMCID: PMC5723461
- DOI: 10.1120/jacmp.v5i2.1947
Stereotactic IMRT for prostate cancer: setup accuracy of a new stereotactic body localization system
Abstract
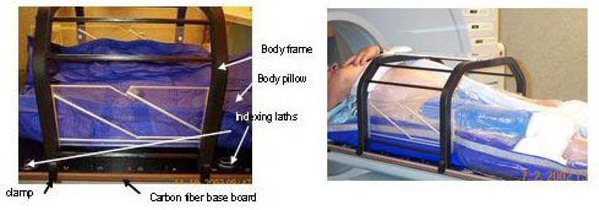
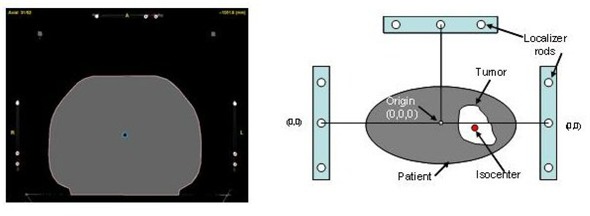
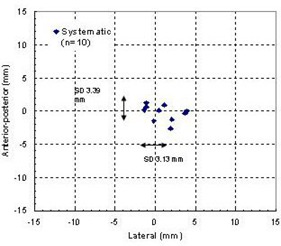
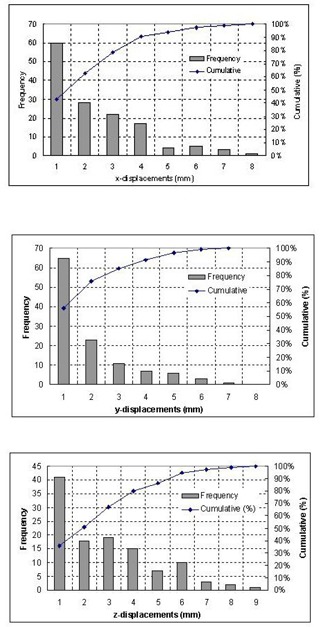
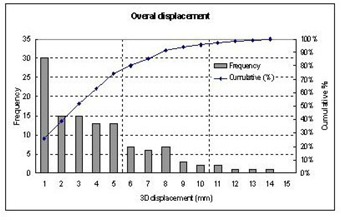
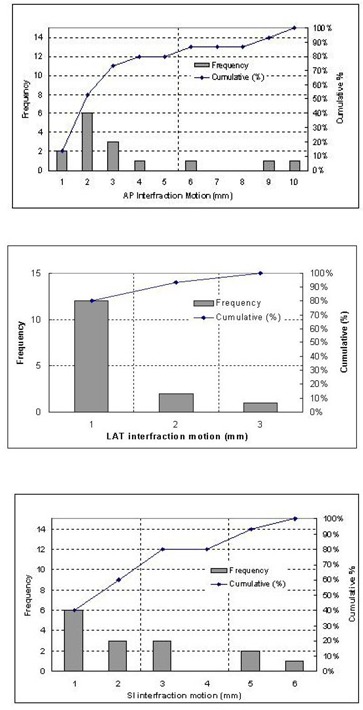
The purpose of this work is to prospectively assess the setup accuracy that can be achieved with a stereotactic body localizer (SBL) in immobilizing patients for stereotactic intensity-modulated radiotherapy (IMRT) for prostate cancer. By quantifying this important factor and target mobility in the SBL, we expect to provide a guideline for selecting planning target volume margins for stereotactic treatment planning. We analyzed data from 40 computed tomography (CT) studies (with slice thickness of 3 mm) involving 10 patients with prostate cancer. Each patient had four sets of CT scans during the course of radiotherapy. For the purpose of this study, all four sets of CT scans were obtained with the patients immobilized in a customized body pillow formed by vacuum suction. Unlike other immobilization devices, this system consists not only of a customized body pillow, but also of a fixation sheet used to suppress patient respiratory motion, a stereotactic body frame to provide stereotaxy, and a carbon fiber base board to which both the body cushion and the frame are affixed. We identified four bony landmarks and measured their coordinates in the stereotactic body frame on each set of CT scans. The displacements of the bony landmarks from their corresponding positions on the simulation scan (first CT scan) were analyzed in three dimensions in terms of overall, systematic, and random categories. The initial planned isocenter was also marked on the patients' skin with fiducials for each CT study. The distance from each bony landmark to the fiducial-based isocenter was measured and compared among the four sets of CT scans. The deviations in distances were also compared to those measured from the landmarks to the stereotactic frame center, in order to determine the effectiveness of the rigid body frame in positioning patients with prostate cancer. Target inter-fraction motion in this system was also studied for five patients by measuring the deviations in distances from the target geometric center to the bony landmarks. Our results showed that the overall setup accuracy had standard deviations (SDs) of 2.58 mm, 2.41 mm, and 3.51 mm in lateral (LAT), anterior-posterior(AP), and superior-inferior (SI) directions, respectively. The random component had SDs of 1.72 mm, 2.06 mm, and 2.79 mm, and the systematic component showed SDs of 0.92 mm, -0.27 mm, and 0.90 mm in these three directions. In terms of three-dimensional vector, the mean displacement over 116 measurements was 3.0 mm with an SD of 1.29 mm. Compared to the rigid reference, the skin-mark-based reference was less reliable for patient repositioning in terms of reproducing known bony landmark positions. The mean target mobility relative to the bony landmarks was 2.22 +/- 3.45 mm, 0.17 +/- 1.11 mm, and 0.11 +/- 2.69 mm in the AP, LAT, and SI directions, respectively. In conclusion, the body immobilization system has the ability to immobilize prostate cancer patients with satisfactory setup accuracy for fractionated extracranial stereotactic radiotherapy. A rigid frame system serves as a reliable alignment reference in terms of repositioning patients into the planning position, while skin-based reference showed larger deviations in repositioning patients.
Figures
Similar articles
-
Repositioning accuracy of a commercially available double-vacuum whole body immobilization system for stereotactic body radiation therapy.Technol Cancer Res Treat. 2004 Feb;3(1):59-67. doi: 10.1177/153303460400300107. Technol Cancer Res Treat. 2004. PMID: 14750894 Clinical Trial.
-
Near simultaneous computed tomography image-guided stereotactic spinal radiotherapy: an emerging paradigm for achieving true stereotaxy.Int J Radiat Oncol Biol Phys. 2003 Nov 1;57(3):605-13. doi: 10.1016/s0360-3016(03)00792-2. Int J Radiat Oncol Biol Phys. 2003. PMID: 14529763
-
[First experiences with a noninvasive patient set-up system for radiotherapy of the prostate].Strahlenther Onkol. 2000 May;176(5):217-22. doi: 10.1007/s000660050003. Strahlenther Onkol. 2000. PMID: 10847118 German.
-
IMRT for prostate cancer: defining target volume based on correlated pathologic volume of disease.Int J Radiat Oncol Biol Phys. 2003 May 1;56(1):184-91. doi: 10.1016/s0360-3016(03)00085-3. Int J Radiat Oncol Biol Phys. 2003. PMID: 12694837 Review.
-
[Conformational radiotherapy in cancers of the prostate: contribution of pelvic immobilization and new fiducial markers].Cancer Radiother. 1997;1(4):307-13. doi: 10.1016/s1278-3218(97)81498-9. Cancer Radiother. 1997. PMID: 9435821 Review. French.
Cited by
-
Commissioning and quality assurance of a commercial stereotactic treatment-planning system for extracranial IMRT.J Appl Clin Med Phys. 2006 Winter;7(1):21-34. doi: 10.1120/jacmp.v7i1.2125. Epub 2006 Feb 15. J Appl Clin Med Phys. 2006. PMID: 16518314 Free PMC article.
-
Feasibility and early clinical assessment of flattening filter free (FFF) based stereotactic body radiotherapy (SBRT) treatments.Radiat Oncol. 2011 Sep 12;6:113. doi: 10.1186/1748-717X-6-113. Radiat Oncol. 2011. PMID: 21910868 Free PMC article.
-
Spine Stereotactic Body Radiation Therapy Residual Setup Errors and Intra-Fraction Motion Using the Stereotactic X-Ray Image Guidance Verification System.Int J Med Phys Clin Eng Radiat Oncol. 2014 Feb;3(1):1-8. doi: 10.4236/ijmpcero.2014.31001. Int J Med Phys Clin Eng Radiat Oncol. 2014. PMID: 29333353 Free PMC article.
-
Intrafractional setup errors in patients undergoing non-invasive fixation using an immobilization system during hypofractionated stereotactic radiotherapy for lung tumors.J Radiat Res. 2013 Jul 1;54(4):762-8. doi: 10.1093/jrr/rrt001. Epub 2013 Feb 14. J Radiat Res. 2013. PMID: 23412467 Free PMC article.
-
PTV margin for dose escalated radiation therapy of prostate cancer with daily on-line realignment using internal fiducial markers: Monte Carlo approach and dose population histogram (DPH) analysis.J Appl Clin Med Phys. 2006 May 25;7(2):38-49. doi: 10.1120/jacmp.v7i2.2210. J Appl Clin Med Phys. 2006. PMID: 17533327 Free PMC article.
References
-
- Verhey L.J., Immobilizing and Positioning Patients for Radiotherapy, Semin. Radiat. Oncol. 5, 100–14 (1995). - PubMed
-
- Pirzkall A., Debus J., Lohr F., Fuss M., Rhein B., Engenhart–Cabillic R., and Wannenmacher M., Radiosurgery alone or in combination with whole‐brain radiotherapy for brain metastases, J. Clin. Oncol. 16, 3563–9 (1998). - PubMed
-
- Hanks G.E., Martz K.L., and Diamond J.J., The effect of dose on local control of prostate cancer, Int. J. Radiat. Oncol. Biol. Phys. 15, 1299–305 (1988). - PubMed
-
- Perez C.A., Bauer M., Edelstein S., Gillespie B.W., and Birch R., Impact of tumor control on survival in carcinoma of the lung treated with irradiation, Int. J. Radiat. Oncol. Biol. Phys. 12, 539–47 (1986). - PubMed
-
- Zelefsky M.J., Leibel S.A., Gaudin P.B., Kutcher G.J., Fleshner N.E., Venkatramen E.S. et al., Dose escalation with three‐dimensional conformal radiation therapy affects the outcome in prostate cancer, Int. J. Radiat. Oncol. Biol. Phys. 41, 491–500 (1998). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
