

Review
doi: 10.1186/1476-7120-3-6.
Ultrasound imaging versus morphopathology in cardiovascular diseases. Coronary collateral circulation and atherosclerotic plaque
Affiliations
- PMID: 15740620
- PMCID: PMC554094
- DOI: 10.1186/1476-7120-3-6
Item in Clipboard
Review
Ultrasound imaging versus morphopathology in cardiovascular diseases. Coronary collateral circulation and atherosclerotic plaque
Cardiovasc Ultrasound.
.
Abstract
This review article is aimed at comparing the results of histopathological and clinical imaging studies to assess coronary collateral circulation in humans. The role of collaterals, as emerging from morphological studies in both normal and atherosclerotic coronary vessels, is described; in addition, present role and future perpectives of echocardiographic techniques in assessing collateral circulation are briefly summarized.
Figures
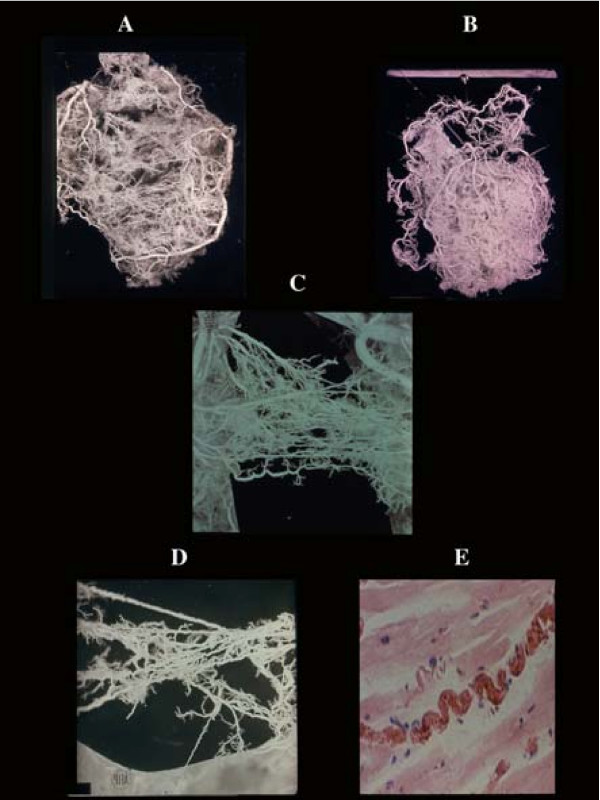
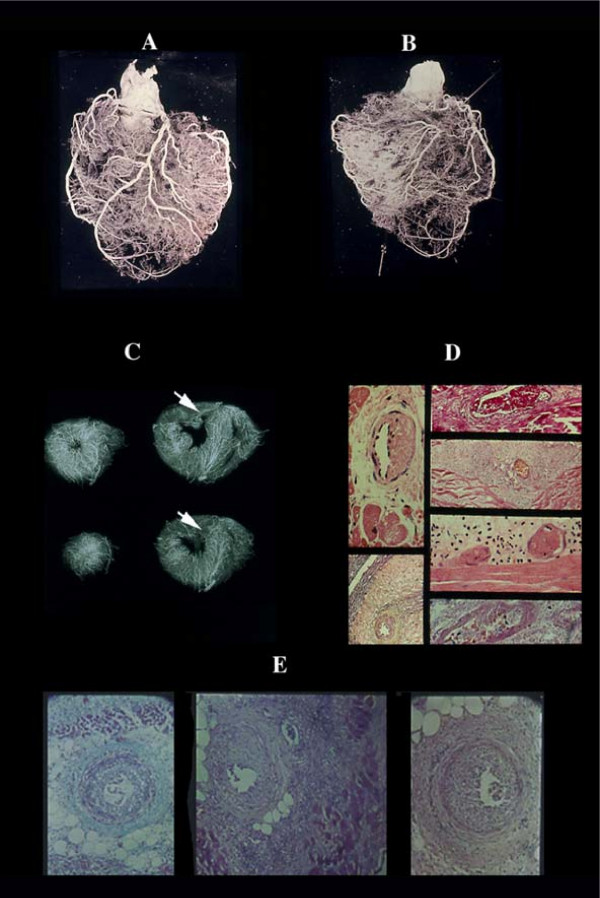
Coronary anastomoses or collaterals. A) intercoronary ventricular and (B), atrial. C) homocoronary anastomoses. Note the innumerous collaterals joining different intramural branches at any level of their course. They have frequently a corkscrew aspect (D) visible also histologically (E), as adaptation to cardiac contraction-relaxation cycle.
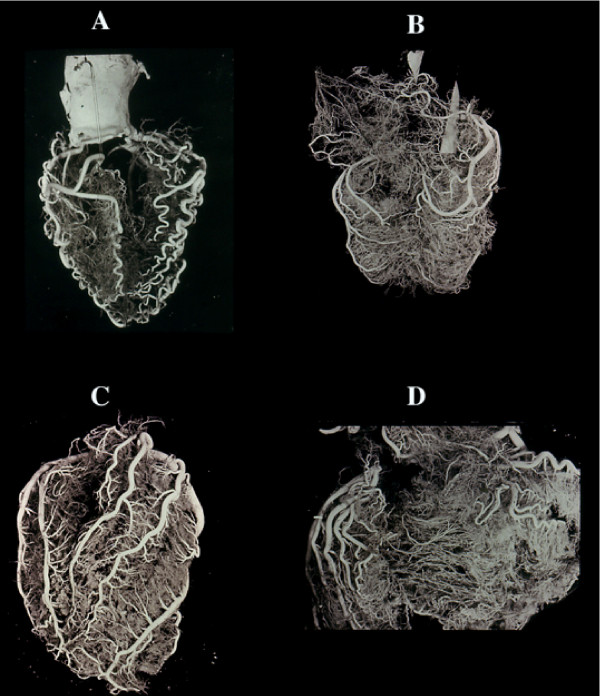
Vessel changes in relation to modification of the cardiac mass. A) atrophic heart with acquired serpentoid form of extramural vessels due to cardiac mass reduction, and minor intramural vascularity. The contrary is seen in cardiac hypertrophy (B) in which the extramural arteries increase in length and diameter (but not in number) to adapt themselves to the greater myocardial mass. Similarly, the same enlargement is seen in the intramural branches. Cor pulmonale, in which condition the right ventricle may become greater than the left one, is an extreme example of adaptation of extramural (C) and intramural, including collaterals (D). No histologic evidence exists of new vessel formation. The cardiac vein show a similar behaviour.
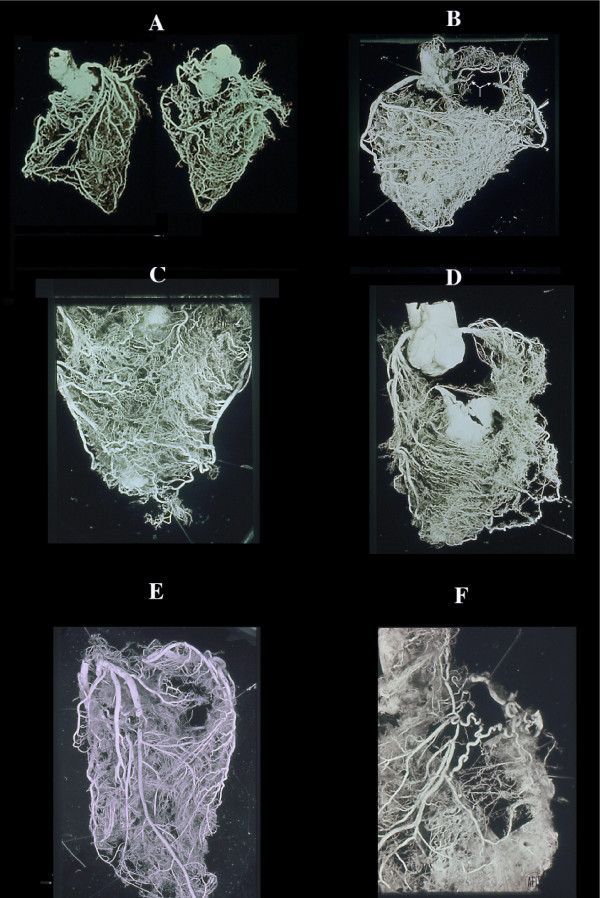
Collateral enlargement in topographical relation (satellite) with severe stenosis or occlusion. A double occlusion of LAD (anterior view) and occlusion of RCA (posterior view) apparently compensated by enlarged collaterals in a non cardiac patient dead from brain hemorrhage. B, similar condition in cases with RCA occlusion (arrow) without corresponding myocardial infarct with numerous homo and intercoronary collaterals of the anterior wall (C), and (D) septum. Occlusion of LAD without evidence of other stenotic changes of the coronary arteries in a 39-year-old woman with rheumatic heart disease and mitral insufficiency. In this case, arteritis was documented histologically by sampling before corrosion. An acute infarct (avascular area at the apex, arrow) was present. F, a single, high enlarged collateral from LCX, supplying the distal tract of an occluded LAD. Note, numerous normal anastomoses. This indicates that ischemia is not the cause (no diffuse enlargement of all collaterals in the whole ischemic area) but rather pressure gradient induces selective compensatory routes.
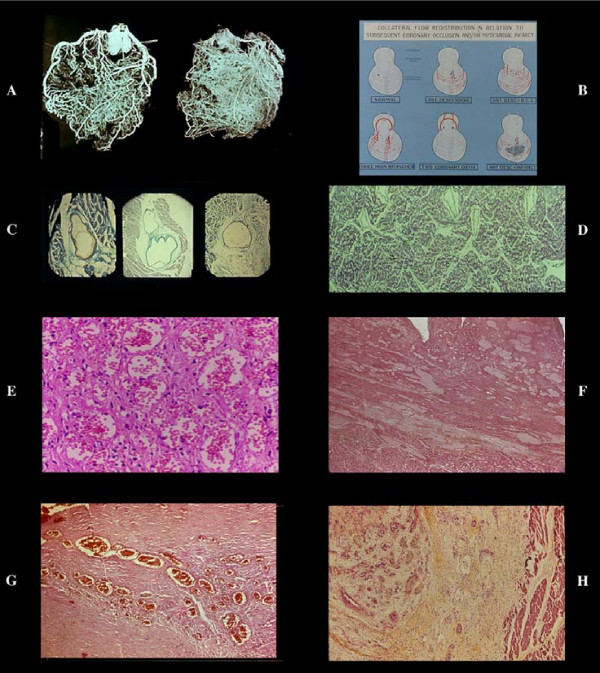
Different aspects of collateral compensation in presence of the same occlusive pattern of LAD. A, relatively few very enlarged collaterals and (B) numerous relatively small collaterals. This divergency may be due to progressive atherosclerotic obstruction of other main vessels or lost of the intramural vasculature, including collaterals, following an infarct. Chart C shows all the possibilities of flow redistribution. The histology of the enlarged anastomoses corresponds to a capillar-like wall, even in the rare extramural collaterals with rudimentary focal tunica media (C). D), enlarged collaterals in a case of anomalous origin of LAD from the pulmonary artery and (E,G) different aspects of giant capillaries (or plexus) in various stages of an acute/old infarction. The absence of new vessel formation is well documented in recent infarcts associated with endocardial thrombus (G). In the latter numerous new vessels form in the granulation tissue repair of the thrombus in contrast to their absence in infarct (arrow; postmortem coronary injection for vessels identification).
Avascular area of an infarct. By plastic cast (A anterior, B posterior view) or postmortem angiogram (C) the infarcted zone (arrow) lacks of intramural vessel injection ("avascular area"). Stretching of the necrotic myocardium and secondary vascular damage with wall degeneration and thrombosis (D), explain this vascular "sequestration" which occurs in early phase. This may indicate a blockage without possibility of therapeutical intervention via blood flow within the infarcted myocardium. Note that the avascular area in this AMI case documented histologically, depended from LAD without evidence of occlusion or severe stenosis. The occluded vessel (arrow) was (B) the RCA, the distal part of which was filled by numerous anastomoses. No myocardial damage was seen in its territory. By dissection even an expert pathologist, the diagnosis could be of myocardial infarction following occlusion of the RCA. E) obliterative intimal hyperplasia in arterioles around a seven days old infarct with early repair process.
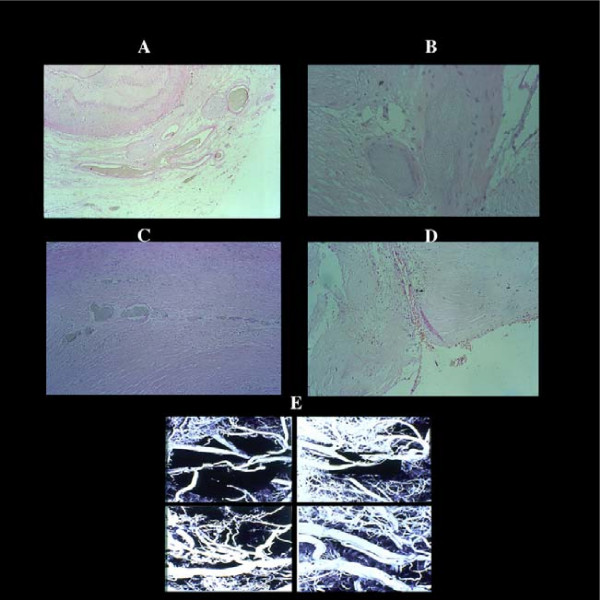
Vascularization of a coronary atherosclerotic plaque showing different aspects of neovascularization. By serial sections of postmortem injected plaques, giant advential capillary-like vessels (A) are connected with secondary branches proximal and distal to the plaque and with new arterioles (B) with a well developed tunica media (indication of functioning blood flow), within the thickened, atherosclerotic intima in turn joined through angiomatous plexuses (C) to the residual lumen (D) E) plastic casts of plaques with different aspects of vascularization.
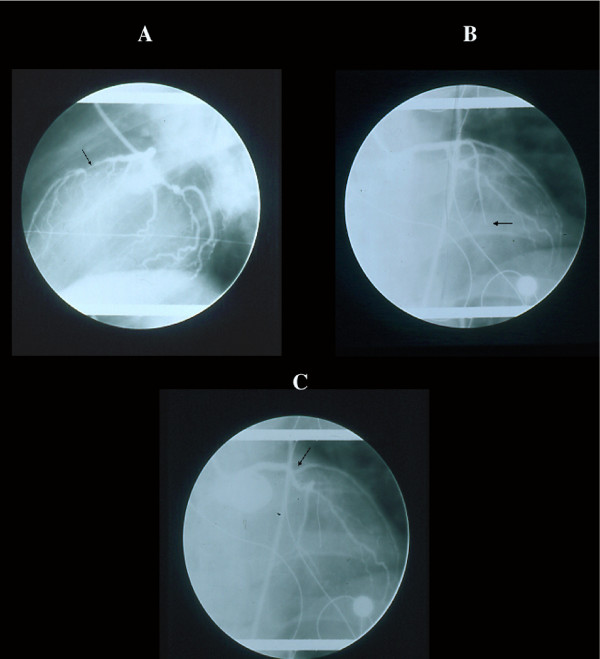
Cineangiographic monitoring in a patient with non occlusive LAD stenosis (A) who developed an extensive infarct without angiographic occlusion. The subsequent imaging of occlusion began distally (B) and ascended to the origin (C) of the vessel (arrow) indicating that the angiographic "pseudocclusion" was due to stasis for increased peripheral resistance and not for primitive thrombosis, not shown morphologically (see text).
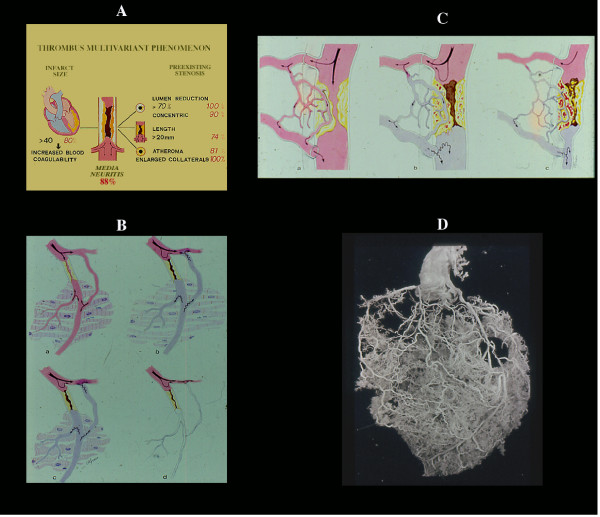
The coronary thrombus is a multivariant phenomenon (A), including medial neuritis. Its location in severe (≥70) stenosis associated with other factors (retrograde collateral flow, reduced fibrinolytic activity, etc, see text) justifies the concept that is a secondary phenomenon. Any time there is an increased peripheral resistance (B) (spasm, intramural extravascular compression following infarction, etc), stasis in related main vessel and in collaterals both outside and within the plaque is expected with hemorrhage, plaque rupture and trombosis (C). On the other hand, it is difficult to accept that acute occlusion of a pin-point lumen bypassed by preexisting functioning collaterals (D) may result in infarct necrosis or sudden death. Even experimentally occlusion of a severe "chronic" (7 days) stenosis does not produce any ischemic dysfunction.
References
-
- Helfant RH, Kemp HG, Gorlin R. The interrelation between extent of coronary artery disease, presence of collaterals, ventriculographic abnormalities and hemodynamics. Am J Cardiol. 1970;25:102. doi: 10.1016/0002-9149(70)90875-1. - DOI
-
- Baroldi G, Mantero O, Scomazzoni G. The collaterals of the coronary arteries in normal and pathologic hearts. Circ Res. 1956;4:223. - PubMed
-
- Baroldi G, Scomazzoni G. American Registry of Pathology, AFIP. Washington D.C., U.S. Government Printing Office; 1967. Coronary Circulation in the Normal and Pathological Heart.
-
- DeWood MA, Spores J, Notske R, Mouser LT, Burroughs R, Golden MS, Lang HT. Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N Engl J Med. 1980;303:897. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
