

Vaccination of metastatic melanoma patients with autologous dendritic cell (DC) derived-exosomes: results of thefirst phase I clinical trial
- PMID: 15740633
- PMCID: PMC554765
- DOI: 10.1186/1479-5876-3-10
Vaccination of metastatic melanoma patients with autologous dendritic cell (DC) derived-exosomes: results of thefirst phase I clinical trial
Abstract
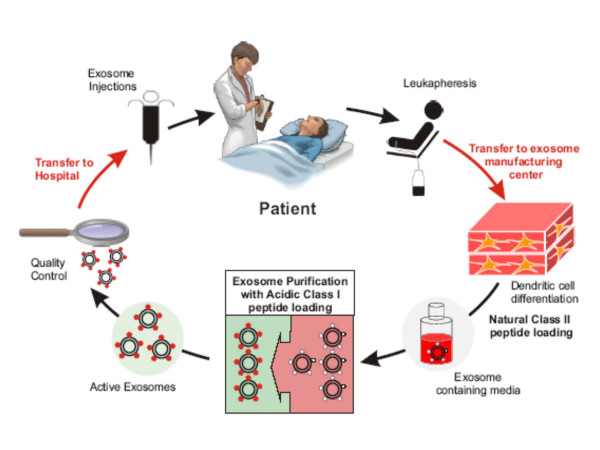
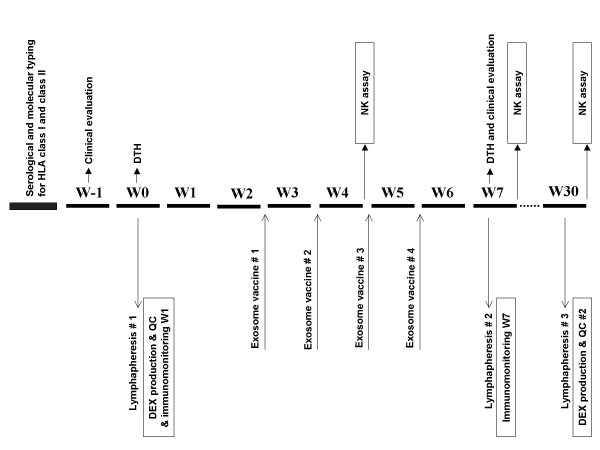
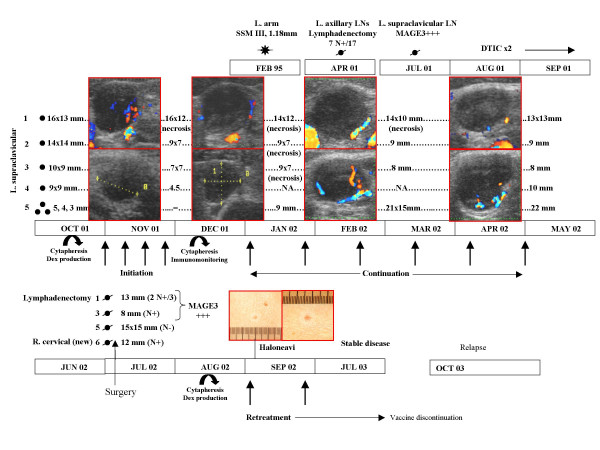
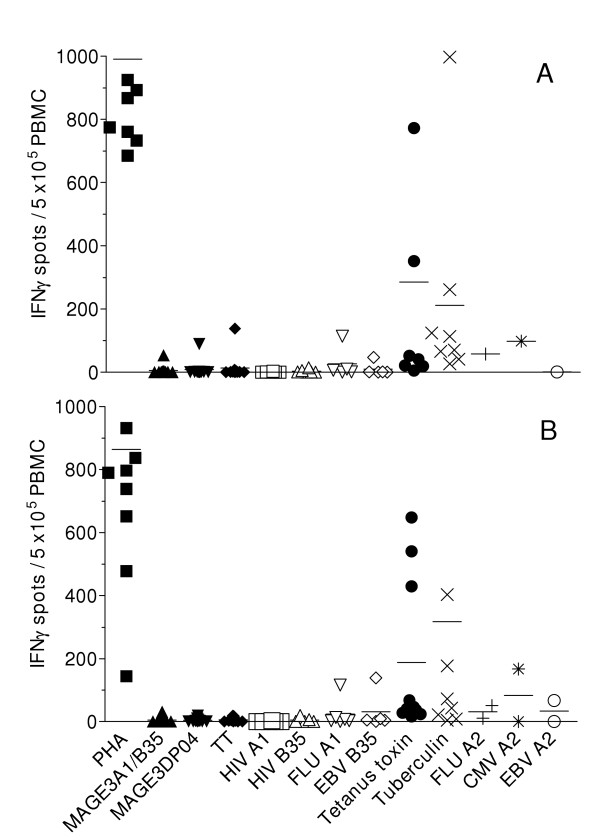
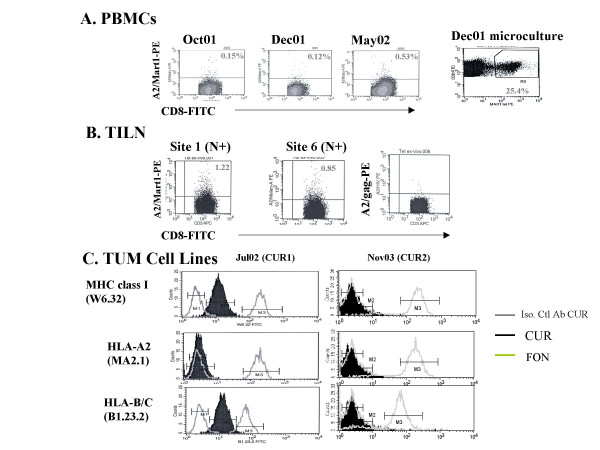
BACKGROUND: DC derived-exosomes are nanomeric vesicles harboring functional MHC/peptide complexes capable of promoting T cell immune responses and tumor rejection. Here we report the feasability and safety of the first Phase I clinical trial using autologous exosomes pulsed with MAGE 3 peptides for the immunization of stage III/IV melanoma patients. Secondary endpoints were the monitoring of T cell responses and the clinical outcome. PATIENTS AND METHODS: Exosomes were purified from day 7 autologous monocyte derived-DC cultures. Fifteen patients fullfilling the inclusion criteria (stage IIIB and IV, HLA-A1+, or -B35+ and HLA-DPO4+ leukocyte phenotype, tumor expressing MAGE3 antigen) were enrolled from 2000 to 2002 and received four exosome vaccinations. Two dose levels of either MHC class II molecules (0.13 versus 0.40 x 1014 molecules) or peptides (10 versus 100 mug/ml) were tested. Evaluations were performed before and 2 weeks after immunization. A continuation treatment was performed in 4 cases of non progression. RESULTS: The GMP process allowed to harvest about 5 x 1014 exosomal MHC class II molecules allowing inclusion of all 15 patients. There was no grade II toxicity and the maximal tolerated dose was not achieved. One patient exhibited a partial response according to the RECIST criteria. This HLA-B35+/A2+ patient vaccinated with A1/B35 defined CTL epitopes developed halo of depigmentation around naevi, a MART1-specific HLA-A2 restricted T cell response in the tumor bed associated with progressive loss of HLA-A2 and HLA-BC molecules on tumor cells during therapy with exosomes. In addition, one minor, two stable and one mixed responses were observed in skin and lymph node sites. MAGE3 specific CD4+ and CD8+ T cell responses could not be detected in peripheral blood. CONCLUSION: The first exosome Phase I trial highlighted the feasibility of large scale exosome production and the safety of exosome administration.
Figures
References
-
- Schuler-Thurner B, Dieckmann D, Keikavoussi P, Bender A, Maczek C, Jonuleit H, Roder C, Haendle I, Leisgang W, Dunbar R, Cerundolo V, von Den Driesch P, Knop J, Brocker EB, Enk A, Kampgen E, Schuler G. Mage-3 and influenza-matrix peptide-specific cytotoxic T cells are inducible in terminal stage HLA-A2.1+ melanoma patients by mature monocyte-derived dendritic cells. J Immunol. 2000;165:3492–3496. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
