

Surgical treatment of aortic abscess and fistula
- PMID: 15745289
- PMCID: PMC548238
Surgical treatment of aortic abscess and fistula
Abstract
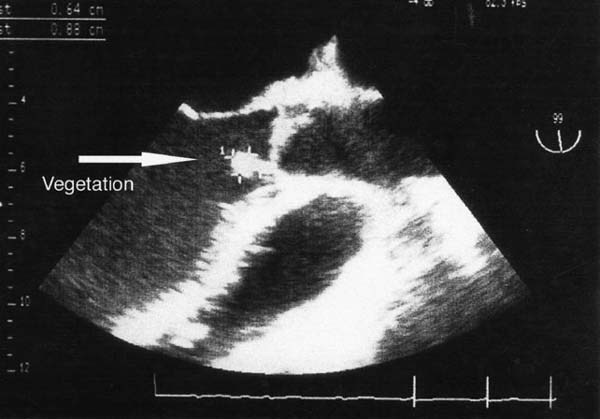
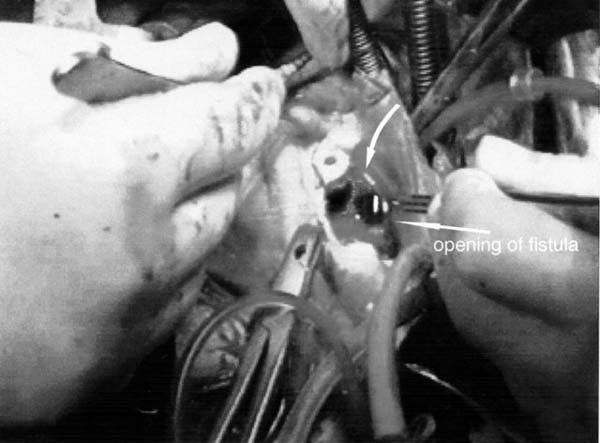
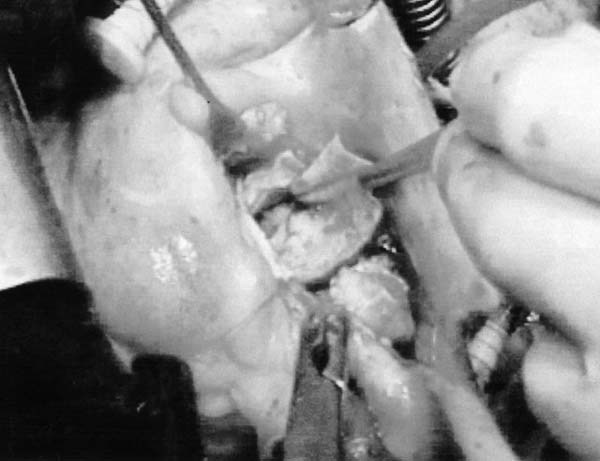
The formation of annular abscess and fistulous communication, the most devastating complication of destructive aortic valve endocarditis, requires extensive surgical débridement. Five men experienced destructive native aortic valve endocarditis in association with congestive heart failure (New York Heart Association functional class IV) and hemodynamic deterioration that developed from severe aortic regurgitation. To eradicate the aortic valve endocarditis, we performed (from July 1998 through November 2002) aortic annular skeletonization by dissecting all infectious and necrotic tissue within the abscess cavity and the fistula between the ventriculoarterial junction and the sinotubular junction. The completely resected annular area was covered with a glutaraldehyde-treated autologous pericardial patch that was sutured firmly to fibrous tissue, for a secure proximal anastomosis. Reconstruction of the aortic root was followed by implantation of a Freestyle stentless bioprosthesis, using the aortic root replacement technique. There were no deaths after surgery, nor is there record of a permanent complication due to a loss of conduction tissue. All 5 patients were in New York Heart Association functional class I or II during follow-up (range, 8-56 months). Echocardiography showed no signs of valve dysfunction, recurrent endocarditis, or fistulation. Annular skeletonization and reconstruction of the aortic annulus with glutaraldehyde-treated autologous pericardium permits radical removal of infected tissue and effective treatment of aortic annular abscess, with less risk of valve dehiscence from the fragile aortic annulus.
Figures
References
-
- d'Udekem Y, David TE, Feindel CM, Armstrong S, Sun Z. Long-term results of operation for paravalvular abscess. Ann Thorac Surg 1996;62:48–53. - PubMed
-
- Knosalla C, Weng Y, Yankah AC, Siniawski H, Hofmeister J, Hammerschmidt R, et al. Surgical treatment of active infective aortic valve endocarditis with associated periannular abscess—11 year results. Eur Heart J 2000;21:490–7. - PubMed
-
- Fiore AC, Ivey TD, McKeown PP, Misbach GA, Allen MD, Dillard DH. Patch closure of aortic annulus mycotic aneurysms. Ann Thorac Surg 1986;42:372–9. - PubMed
-
- David TE, Komeda M, Brofman PR. Surgical treatment of aortic root abscess. Circulation 1989;80(3 Pt 1):I269–74. - PubMed
-
- Endo M, Nishida H, Imamura E, Koyanagi H. Sutureless aortic valve replacement for periannular abscess due to active bacterial endocarditis: a new translocation technique. Ann Thorac Surg 1988;45:568–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical