

Aggressive retinal astrocytomas in four patients with tuberous sclerosis complex
- PMID: 15747752
- PMCID: PMC1280094
Aggressive retinal astrocytomas in four patients with tuberous sclerosis complex
Abstract
Objective: To report the clinical and histopathologic findings of retinal astrocytic tumors that showed progressive growth in four patients with tuberous sclerosis complex (TSC).
Methods: Four young children each developed an enlarging retinal neoplasm that eventually necessitated enucleation of the affected eye. The systemic findings, clinical course, and histopathologic findings were reviewed.
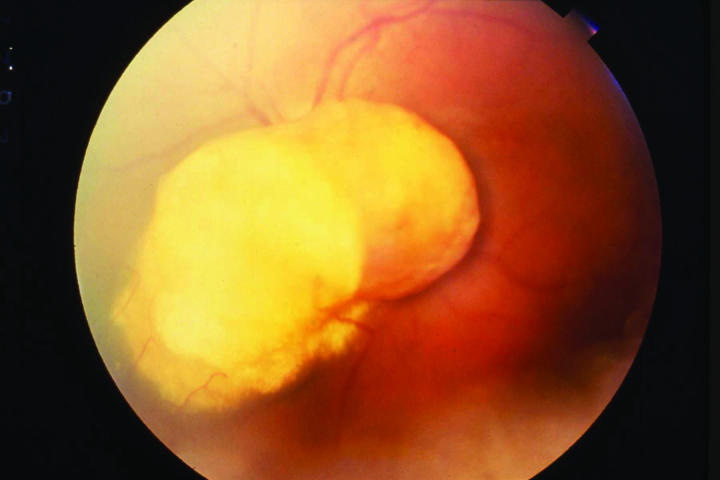
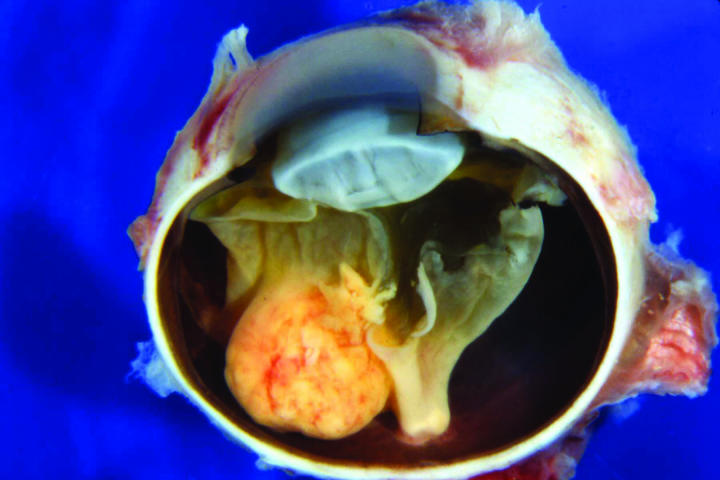
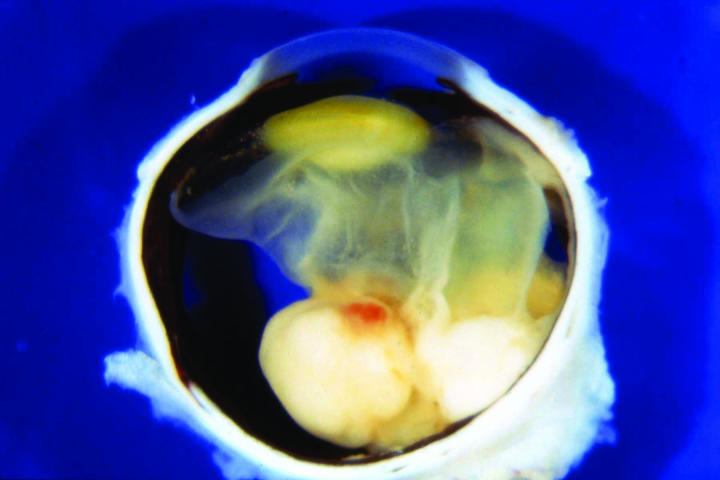
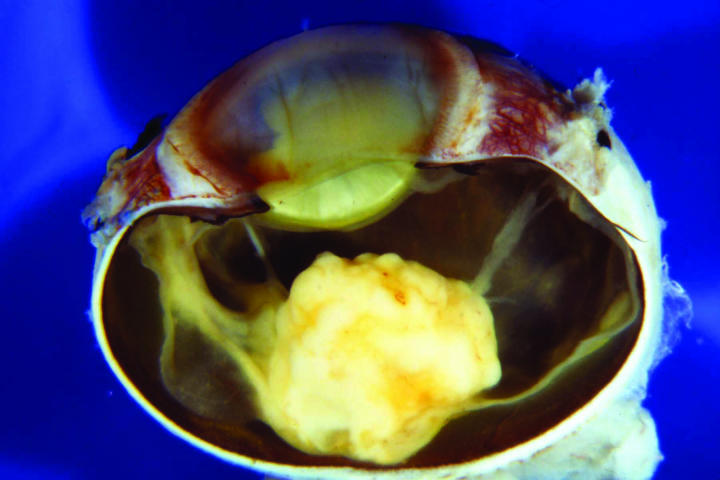
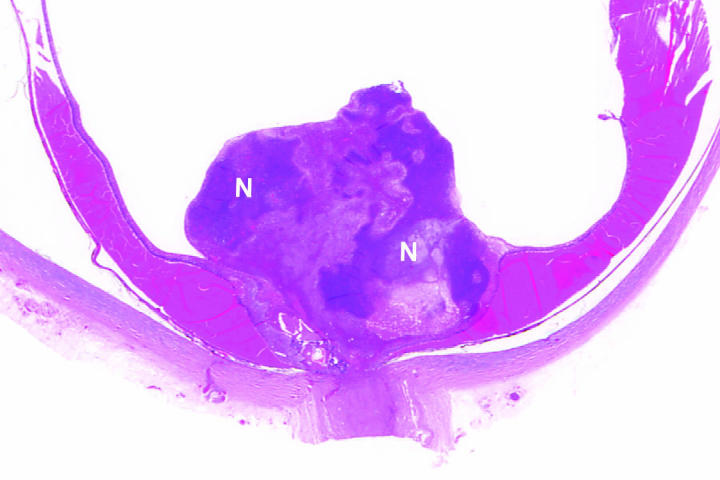
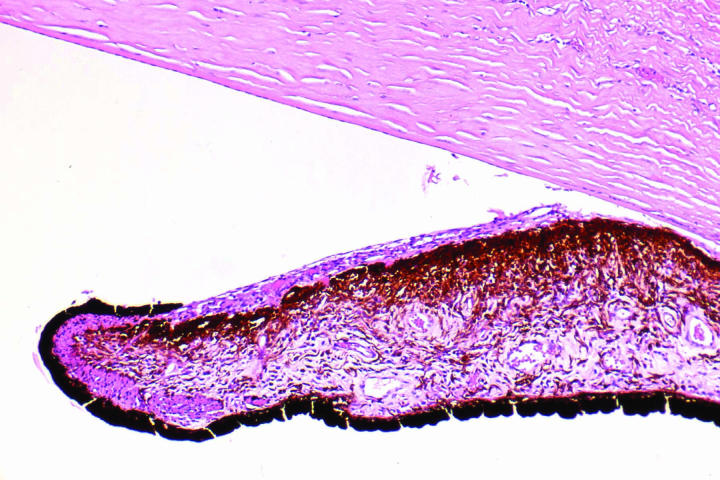
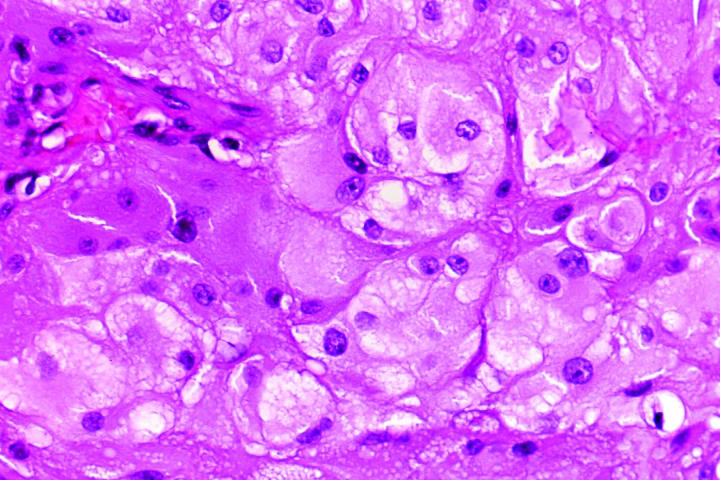
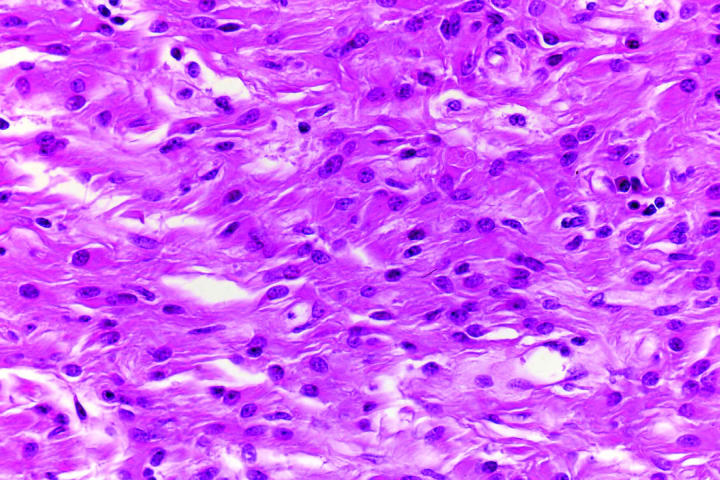
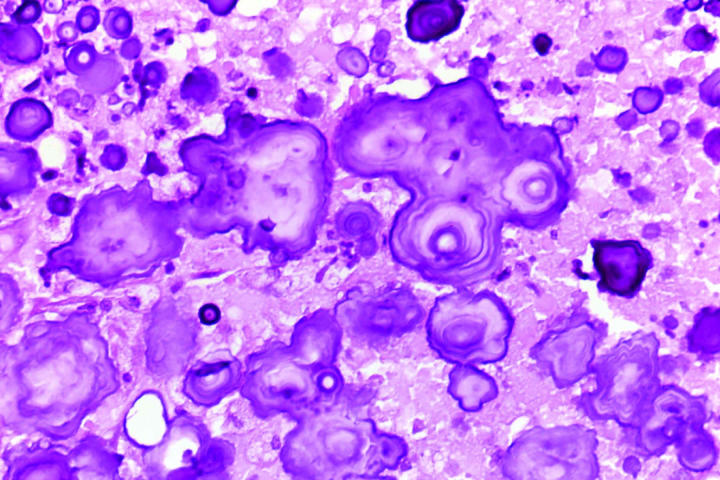
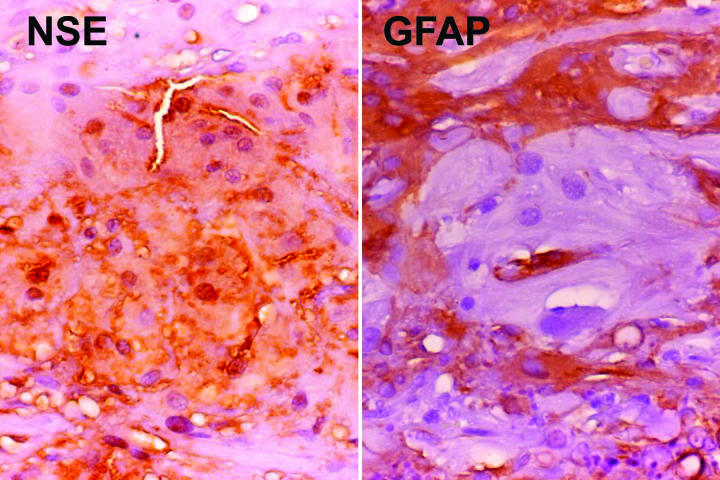
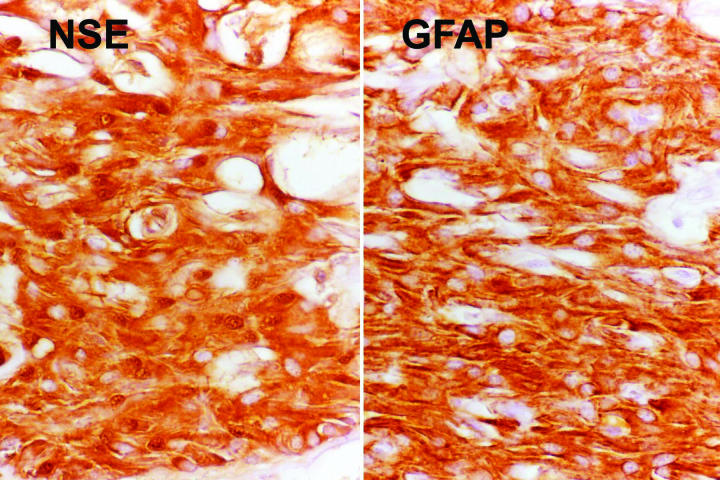
Results: Each patient had a progressively enlarging retinal mass associated with a total exudative retinal detachment and neovascular glaucoma. Enucleation was necessary in each case because the affected eye became blind and painful. The mean patient age at enucleation was 7 years, and the median age was 3 years. At the time of enucleation the tumors ranged from 10 to 20 mm in basal diameter and from 10 to 25 mm in thickness. Histopathologic studies of each eye revealed a giant cell astrocytoma that had produced a total exudative retinal detachment. The tumor cells showed positive immunoreactivity to neuron-specific enolase and glial fibrillary acidic protein. The retinal neoplasms in these cases were identical histopathologically to the subependymal giant cell astrocytoma that typifies TSC in the brain. One tumor filled the entire eye and perforated the globe. Although the lesions simulated retinoblastoma clinically, each patient had ocular and systemic findings of TSC, supporting the diagnosis of astrocytic hamartoma.
Conclusions: Although retinal astrocytic lesions of TSC generally are stationary, they can sometimes grow relentlessly and cause severe ocular complications. Patients with retinal astrocytic hamartomas should have serial ophthalmic evaluations because of this possibility.
Figures

References
-
- Shepherd CW, Scheithauer BW, Gomez MR, et al. Subependymal giant cell astrocytoma: a clinical, pathological, and flow cytometric study. Neurosurgery. 1991;28:864–868. - PubMed
-
- Scheithauer BW and Reagan TJ. Neuropathology, Chapter 9. In: Gomez MR, Sampson JR, Whittemore VH, ed. Tuberous Sclerosis Complex, 3rd Edition. New York: Oxford University Press; 1999:101–144.
-
- Shepherd CW, Beard CM, Gomez MR, et al. Tuberous sclerosis complex in Olmsted County, Minnesota 1950–1989. Arch Neurol. 1991;48:400–401. - PubMed
-
- Nyboer JH, Robertson DM, Gomez MR. Retinal lesions in tuberous sclerosis. Arch Ophthalmol. 1976;94:1277–1980. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
