

Graded partial tenotomy of vertical rectus muscles for treatment of hypertropia
- PMID: 15747755
- PMCID: PMC1280097
Graded partial tenotomy of vertical rectus muscles for treatment of hypertropia
Abstract
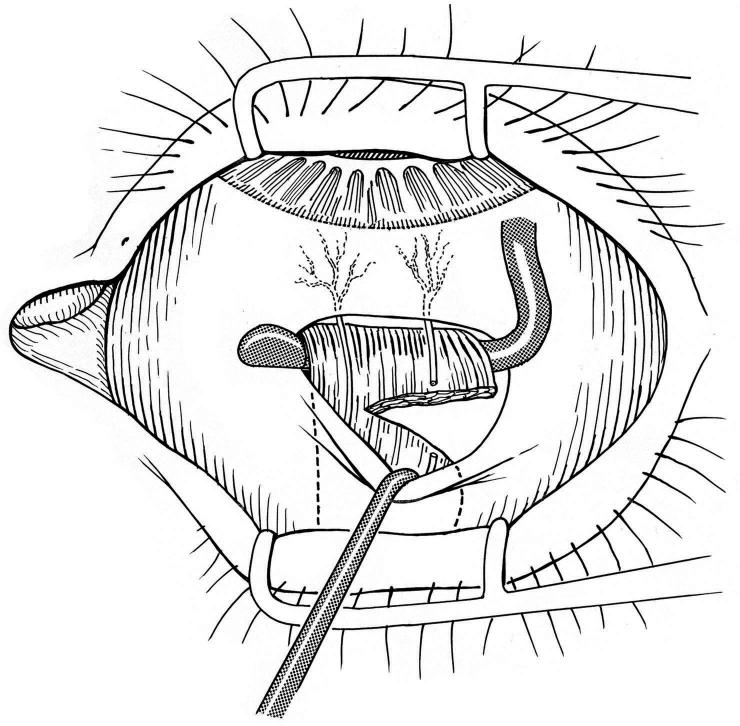
Purpose: To evaluate the effectiveness of graded (adjustable intraoperatively) partial vertical rectus muscle tenotomy at the insertion in correcting small degrees of hypertropia.
Methods: All patients with best-corrected visual acuity of better than 6/30 in both eyes who over a 30-month period underwent partial tenotomy of vertical rectus muscle(s) only (no concurrent oblique muscles) were included. Improvement was evaluated 6 weeks postoperatively as change in alignment in prism diopters (PD) in primary gaze and in the field of action of the affected rectus muscle(s). Binocular function was evaluated by Titmus stereoacuity and the Worth 4-light tests.
Results: All 24 patients who met criteria for inclusion had diplopia preoperatively versus seven patients (29%) postoperatively (P < .005, Student's paired t test). Prisms were used by six preoperatively versus two postoperatively (P < .05, Student's paired t test). The average vertical deviation in primary gaze decreased from 8 PD to 2 PD (P < .005, Student's paired t test). In the field of action of the treated rectus muscle, hypertropia decreased from an average of 8 PD to 3 PD (P < .005, Student's paired t test). For the preoperative and the postoperative assessments available, stereoacuity improved after 10 (56%) of the 18 procedures and Worth 4-light testing showed improvement or maintenance of fusion after 15 (79%) of 19 procedures.
Conclusions: Graded vertical rectus partial tenotomy can effectively reduce small degrees of hypertropia and associated diplopia, improve binocular function, and reduce or eliminate the need for prism correction.
Figures
References
-
- Nemet P, Stolovich C. Biased resection of the medial recti; a new surgical approach to convergence insufficiency. Binocul Vis Strabismus Q. 1990;5:213.
-
- Nemet P, Stolovich C, Lowenstein A. A new operation: slanted (reinsertion) medial rectus muscle surgery for convergence excess esotropia: Results in 12 cases. Binocul Vis Strabismus Q. 1993;8:241.
-
- Biglan AW, Walden P. Results following management of oculomotor nerve palsy with a modified Knapp procedure. Ophthalmic Surg. 1985;16:759–764. - PubMed
-
- von Noorden GK. Examination of the patient. II. Motor signs in heterophoria and heterotropia. In: von Noorden GK, Campos EC, eds. Binocular Vision and Ocular Motility, Theory and Management of Strabismus. Philadelphia: Mosby; 2002:202–206.
-
- Scott AB. Graded rectus muscle tenotomy for small deviations. In: Proceedings of the Jampolsky Festschrift. San Francisco: The Smith-Kettlewell Eye Research Institute; 2000:215–216.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
