

Anterior lens capsule management in pediatric cataract surgery
- PMID: 15747769
- PMCID: PMC1280111
Anterior lens capsule management in pediatric cataract surgery
Abstract
Purpose: To describe and analyze pediatric anterior capsulotomy techniques and make recommendations.
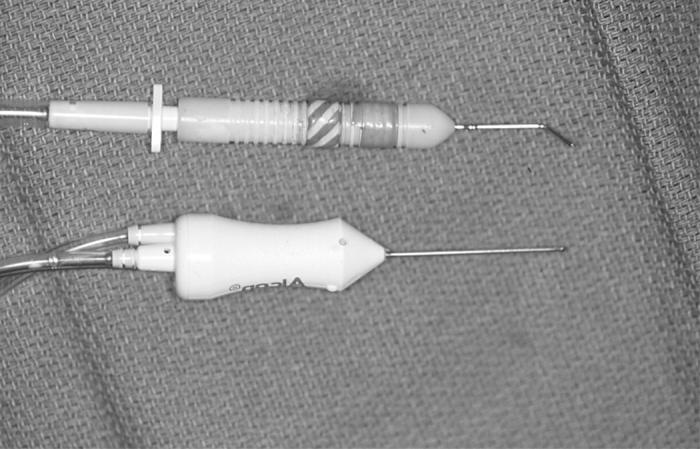
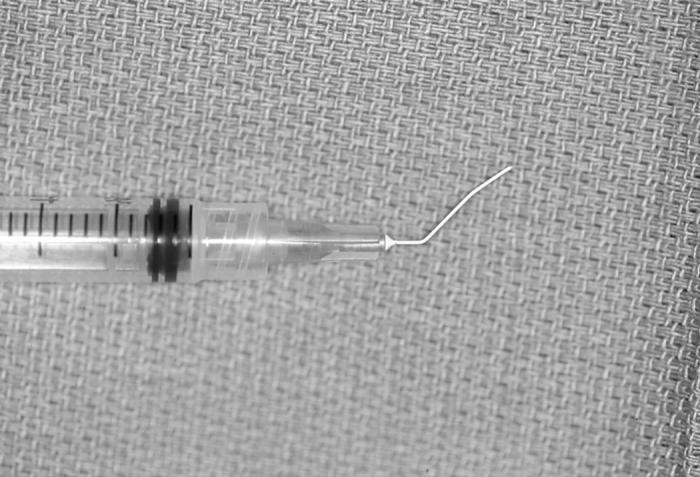
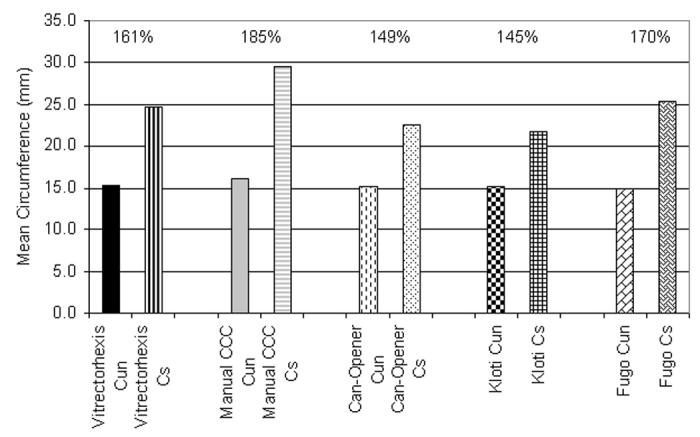
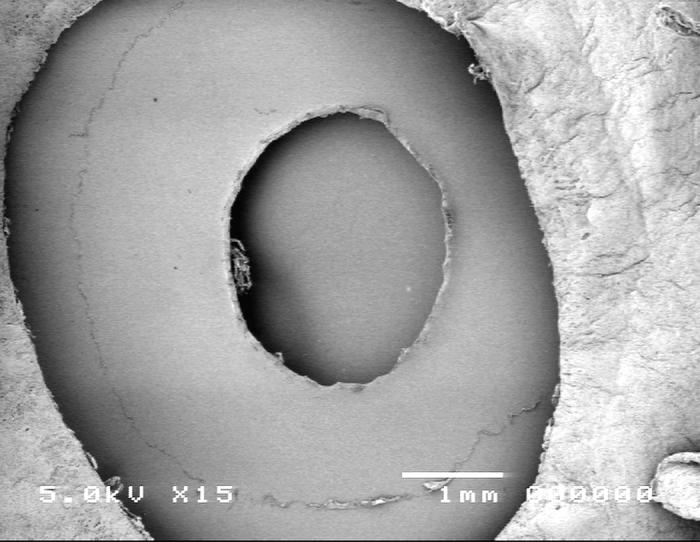
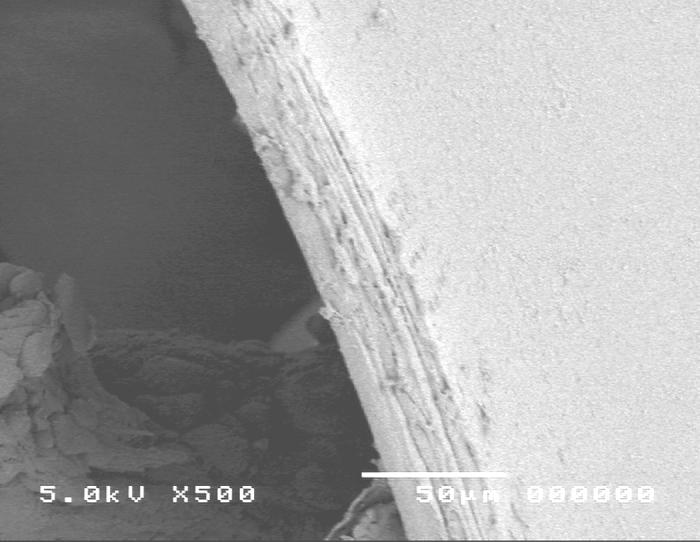
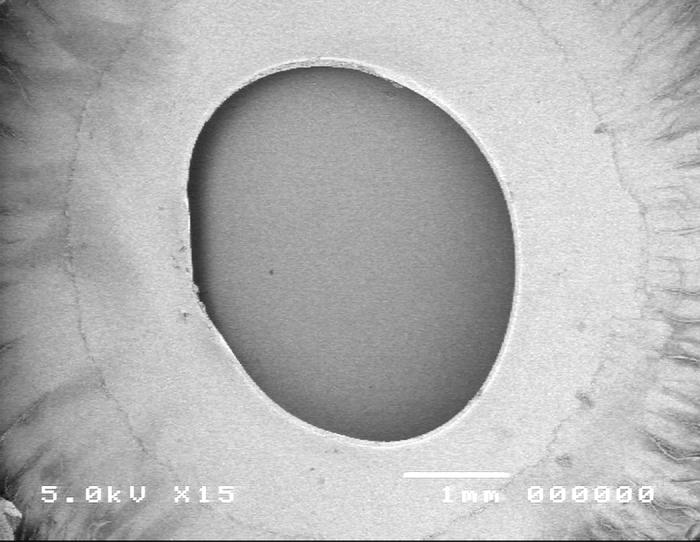
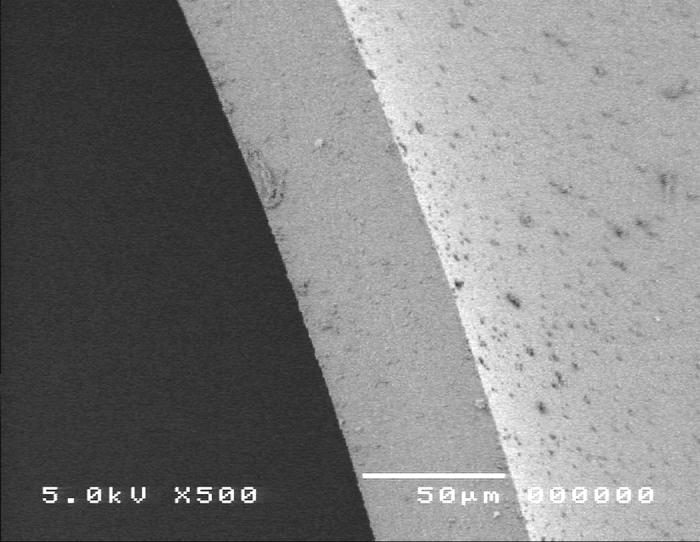
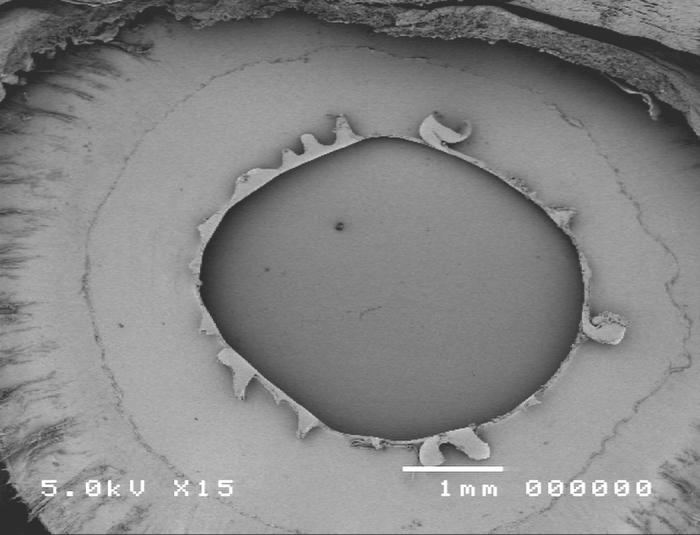
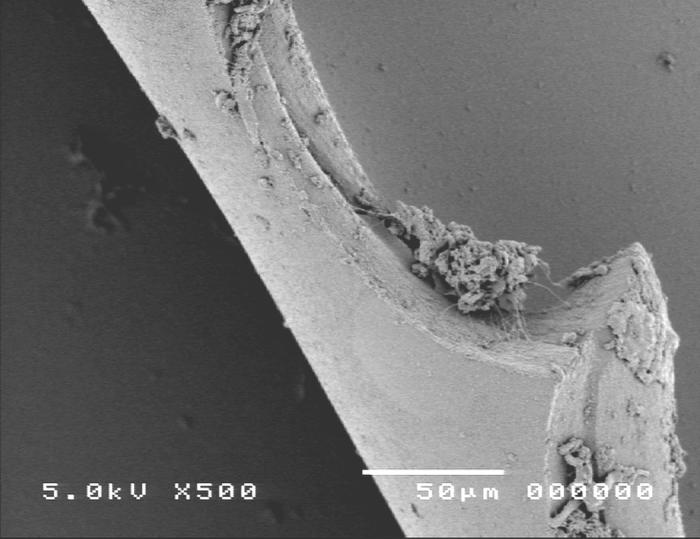
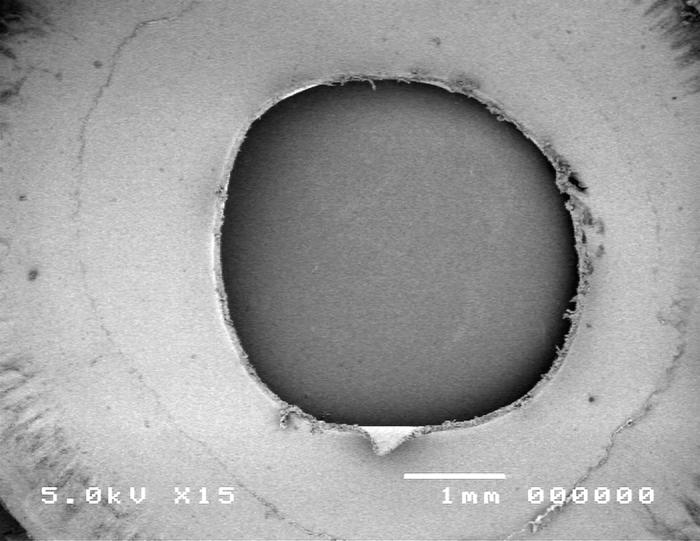
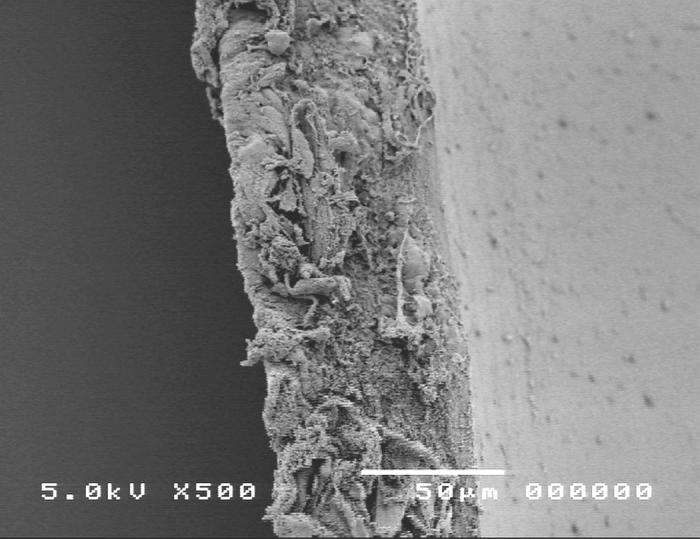
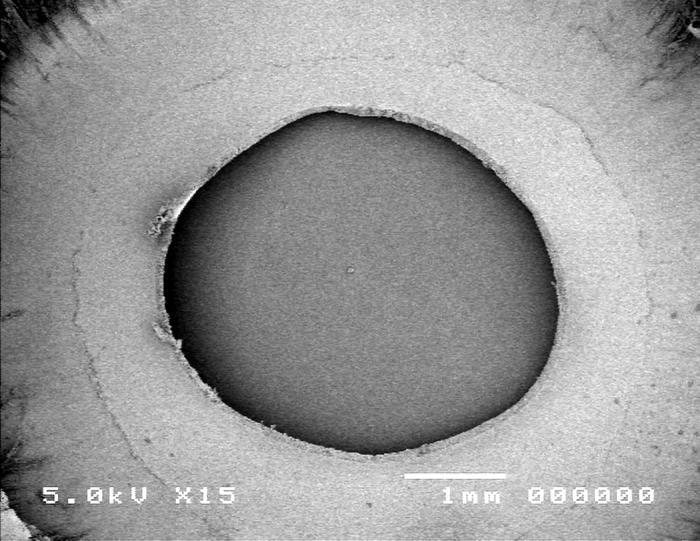
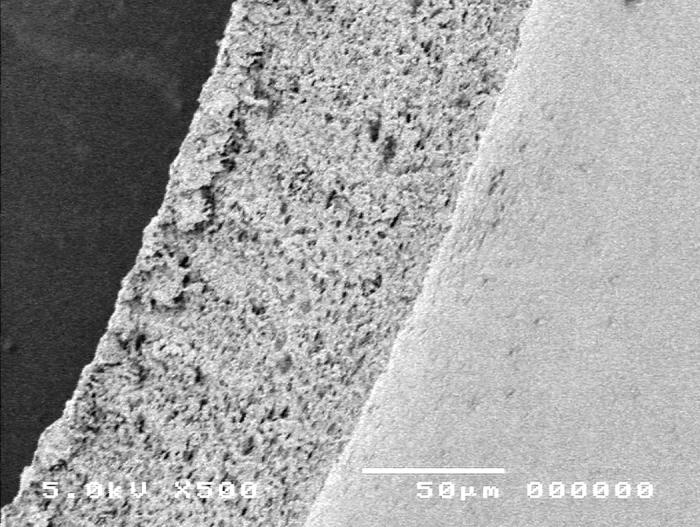
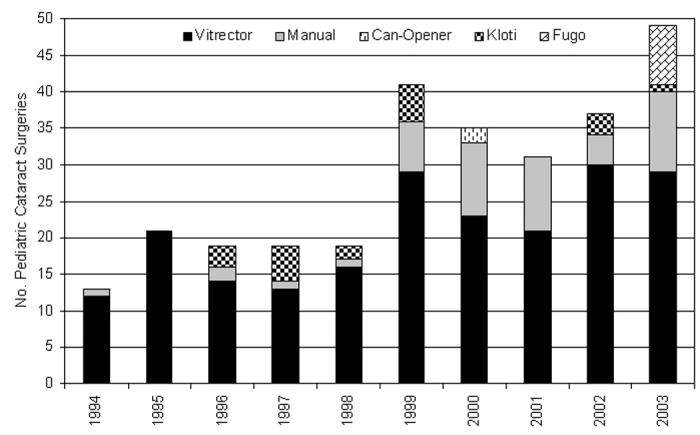
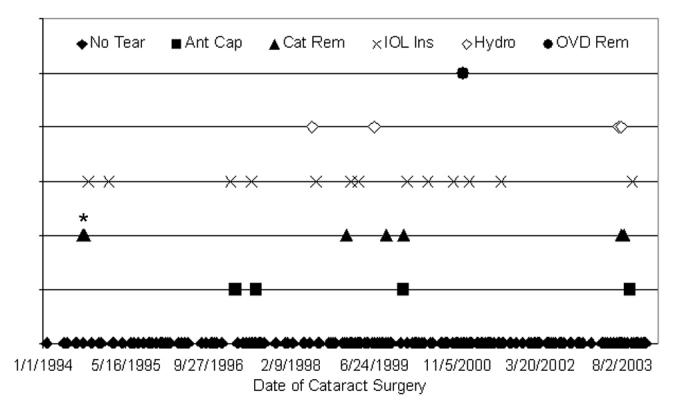
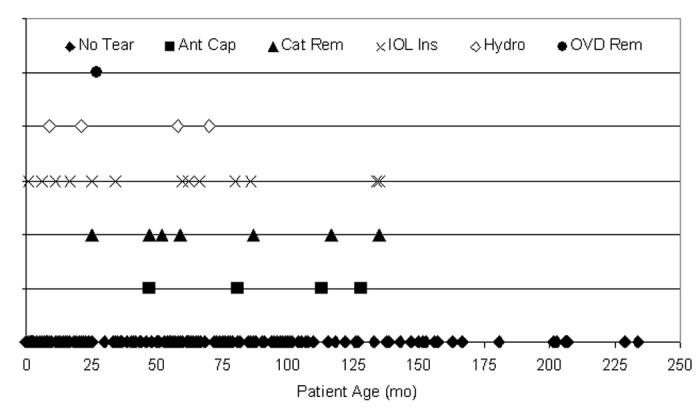
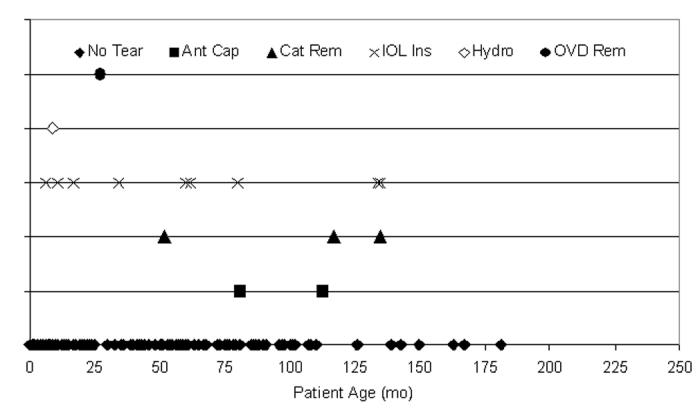
Methods: Five anterior capsulotomy techniques were compared using a porcine model. Extensibility was measured by calculating the mean stretch-to-rupture circumference of each capsulotomy (20 eyes per technique) as a percentage of its circumference at rest. Edge characteristics were reviewed using scanning electron microscopy. A 10-year review of consecutive pediatric cataract surgeries performed by the author focused on the anterior capsulotomy results. A worldwide survey was used to determine current practice patterns.
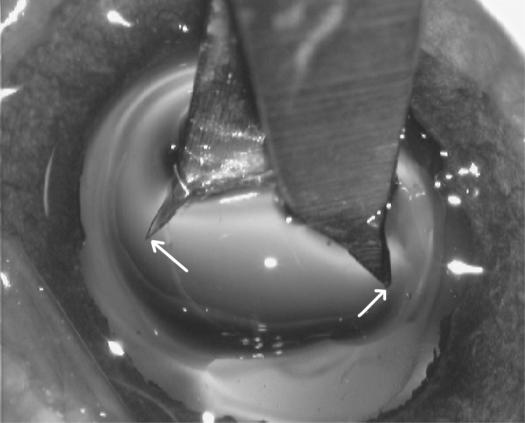
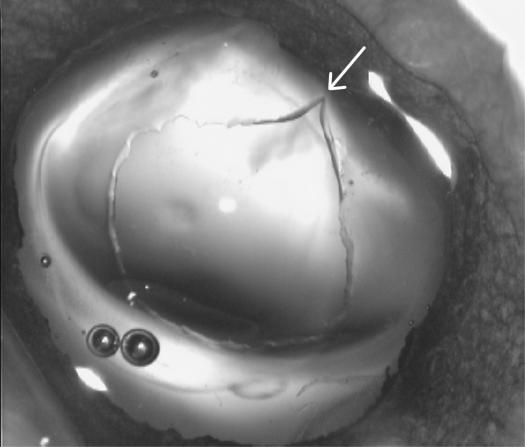
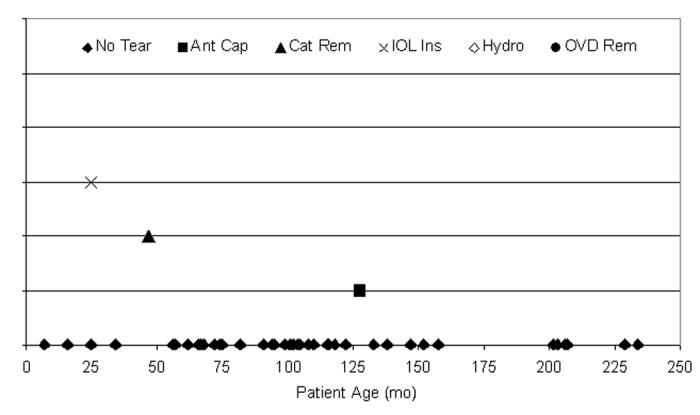
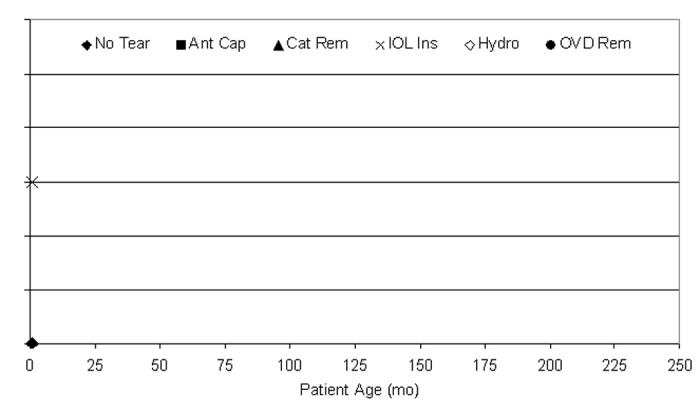
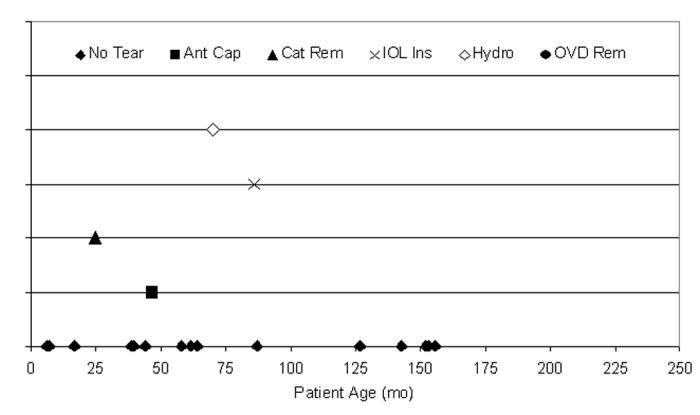
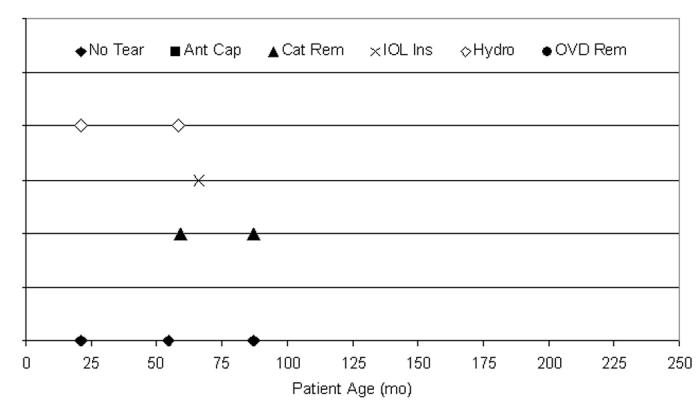
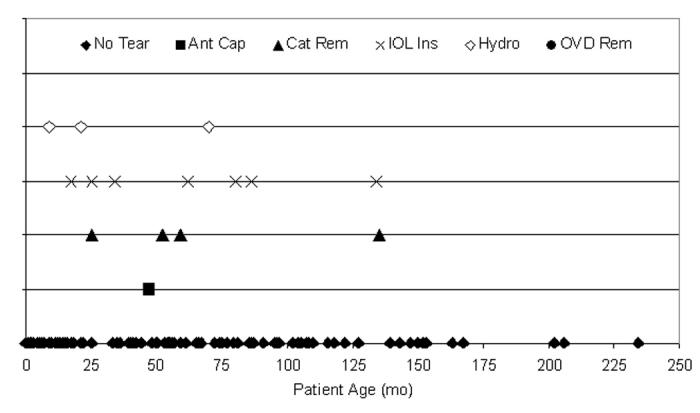
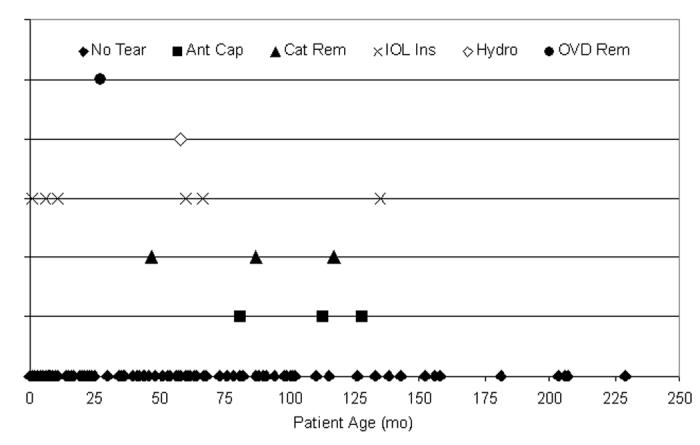
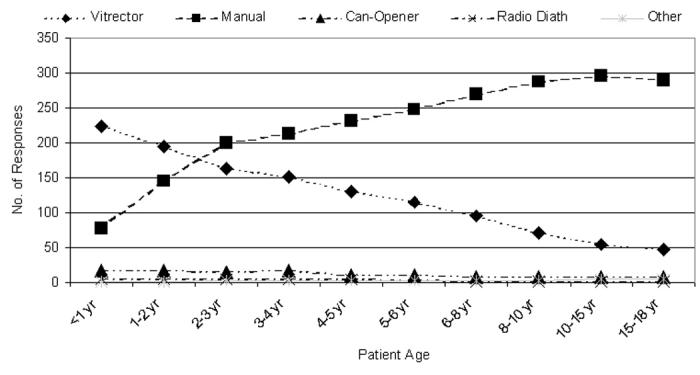
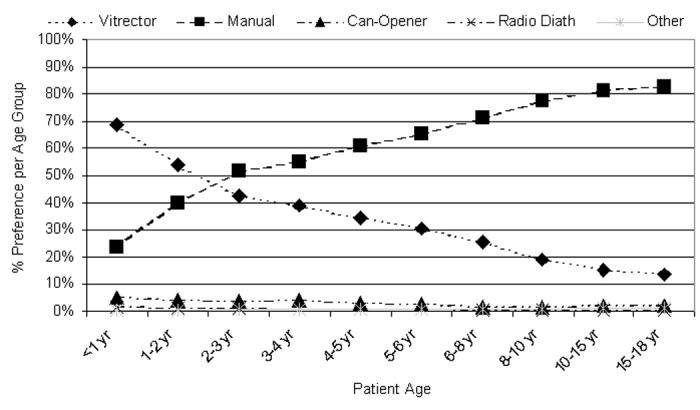
Results: Manual continuous curvilinear capsulorrhexis (CCC) produced the most extensible porcine capsulotomy (185%) with the most regular edge and is preferred by surgeons for patients aged 2 years and older. In the pseudophakic clinical cases reviewed, a radial tear developed in 3 (6.5%) of 46 manual CCC cases. Vitrectorhexis (porcine extensibility, 161%) is preferred by surgeons during the first 2 years of life. A radial tear developed in 16 (7.7%) of 208 vitrectorhexis pseudophakic eyes (29 tears in 284 pseudophakic eyes [10.2%] overall). The Kloti diathermy unit, Fugo plasma blade, and "can-opener" technique produced porcine capsulotomies of 145%, 170%, and 149% extensibility, respectively, and radial tears numbering 4 (21%) of 19, 5 of 8, and 1 of 2, respectively, in the clinical series.
Conclusions: All five capsulotomy techniques are recommendable for children. Only the vitrectorhexis and manual CCC are commonly used today. Vitrectorhexis is well suited for use in infants and young children; manual CCC is best used beyond infancy, and it produces the most stable edge.
Figures






References
-
- Resnikoff S, Kocur I. World sight day: 10 October. World Health Organ 2002. Available at: <http://www.who.int/mediacentre/news/releases/pr79/en/>.
-
- Foster A, Gilbert C, Rahi J. Epidemiology of cataract in childhood: a global perspective. J Cataract Refract Surg. 1997;23:601–604. - PubMed
-
- Ahmad K. WHO launches international programme to combat childhood blindness. Lancet. 2002;359:2258. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
