

A randomized effectiveness trial of cognitive-behavioral therapy and medication for primary care panic disorder
- PMID: 15753242
- PMCID: PMC1237029
- DOI: 10.1001/archpsyc.62.3.290
A randomized effectiveness trial of cognitive-behavioral therapy and medication for primary care panic disorder
Abstract
Background: Panic disorder is a prevalent, often disabling condition among patients in the primary care setting. Although numerous studies have assessed the effectiveness of treatments for depression in primary care, few such studies have been conducted for panic disorder.
Objective: To implement and test the effectiveness of a combined pharmacotherapy and cognitive-behavioral intervention for panic disorder tailored to the primary care setting.
Design: Randomized, controlled study comparing intervention to treatment as usual.
Setting: Six primary care clinics associated with 3 university medical schools, serving an ethnically and socioeconomically diverse patient population.
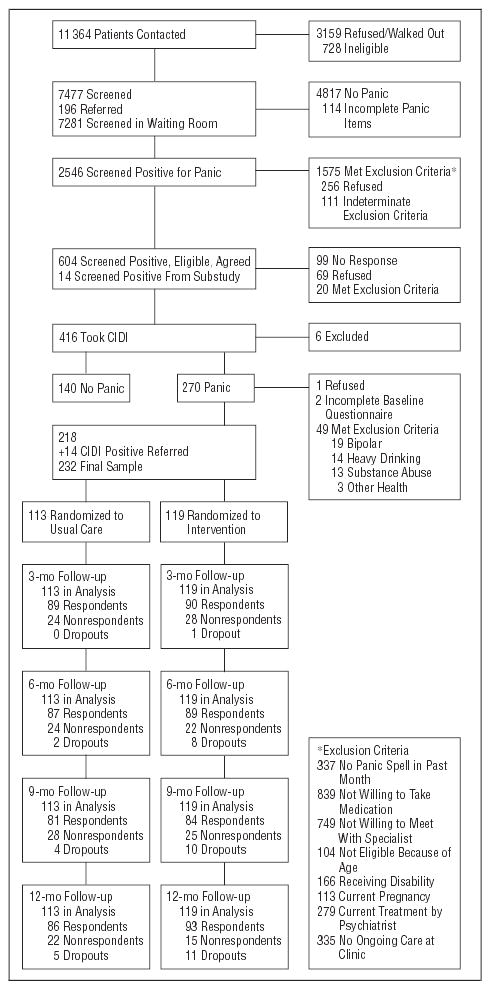
Participants: Two hundred thirty-two primary care patients meeting DSM-IV criteria for panic disorder. Comorbid mental and physical disorders were permitted, provided these did not contraindicate the treatment to be provided and were not acutely life threatening.
Intervention: Patients were randomized to receive either treatment as usual or an intervention consisting of a combination of up to 6 sessions (across 12 weeks) of cognitive-behavioral therapy (CBT) modified for the primary care setting, with up to 6 follow-up telephone contacts during the next 9 months, and algorithm-based pharmacotherapy provided by the primary care physician with guidance from a psychiatrist. Behavioral health specialists, the majority inexperienced in CBT for panic disorder, were trained to deliver the CBT and coordinated overall care, including pharmacotherapy.
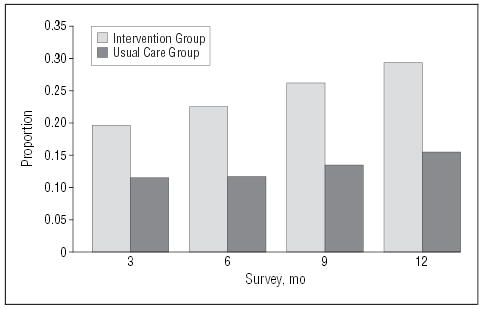
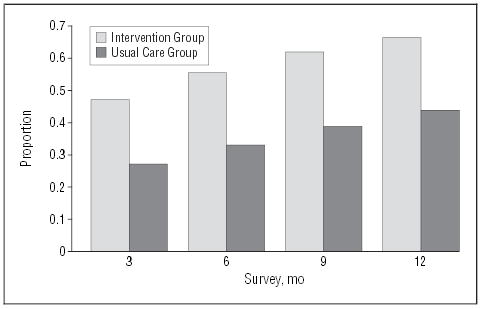
Main outcomes measures: Proportion of subjects remitted (no panic attacks in the past month, minimal anticipatory anxiety, and agoraphobia subscale score <10 on Fear Questionnaire) and responding (Anxiety Sensitivity Index score <20) and change over time in World Health Organization Disability Scale and short form 12 scores.
Results: The combined cognitive-behavioral and pharmacotherapeutic intervention resulted in sustained and gradually increasing improvement relative to treatment as usual, with significantly higher rates at all points of both the proportion of subjects remitted (3 months, 20% vs 12%; 12 months, 29% vs 16%) and responding (3 months, 46% vs 27%; 12 months, 63% vs 38%) and significantly greater improvements in World Health Organization Disability Scale (all points) and short form 12 mental health functioning (3 and 6 months) scores. These effects were obtained in spite of similar rates of delivery of guideline-concordant pharmacotherapy to the 2 groups.
Conclusion: Delivery of evidence-based CBT and medication using the collaborative care model and a CBT-naive, midlevel behavioral health specialist is feasible and significantly more effective than usual care for primary care panic disorder.
Figures
Comment in
-
Coordinated care consisting of cognitive behavioural therapy plus medication improves panic disorder.Evid Based Ment Health. 2005 Nov;8(4):110. doi: 10.1136/ebmh.8.4.110. Evid Based Ment Health. 2005. PMID: 16246886 No abstract available.
References
-
- Katon W, von Korff M, Lin EH, Walker E, Simon GE, Bush T, Robinson P, Russo J. Collaborative management to achieve treatment guidelines: impact on depression in primary care. JAMA. 1995;273:1026–1031. - PubMed
-
- Katon W, Robinson P, Von Korff M, Lin E, Bush T, Ludman E, Simon G, Walker E. A multifaceted intervention to improve treatment of depression in primary care. Arch Gen Psychiatry. 1996;53:924–932. - PubMed
-
- Wells KB, Sherbourne C, Schoenbaum M, Duan N, Meredith L, Unutzer J, Miranda J, Carney MF, Rubenstein LV. Impact of disseminating quality improvement programs for depression in managed primary care: a randomized controlled trial. JAMA. 2000;283:212–220. - PubMed
-
- Unutzer J, Katon K, Callahan CM, Williams JW, Jr, Hunkeler E, Harpole L, Hoffing M, Della Penna RD, Noel PH, Lin EH, Arean PA, Hegel MT, Tang L, Belin TR, Oishi S, Langston C. IMPACT Investigators. Improving mood-promoting access to collaborative treatment: collaborative care management of late-life depression in the primary care setting. JAMA. 2002;288:2836–2845. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MH57858/MH/NIMH NIH HHS/United States
- R01 MH058915/MH/NIMH NIH HHS/United States
- K24 MH065324/MH/NIMH NIH HHS/United States
- MH065324/MH/NIMH NIH HHS/United States
- R01 MH057858/MH/NIMH NIH HHS/United States
- K24 MH064122/MH/NIMH NIH HHS/United States
- U01 MH058915/MH/NIMH NIH HHS/United States
- MH64122/MH/NIMH NIH HHS/United States
- R01 MH057835/MH/NIMH NIH HHS/United States
- MH58915-03/MH/NIMH NIH HHS/United States
- U01 MH057858/MH/NIMH NIH HHS/United States
- U01 MH057835/MH/NIMH NIH HHS/United States
- MH57835/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
