

Relationship between symptoms and disordered continence mechanisms in women with idiopathic faecal incontinence
- PMID: 15753542
- PMCID: PMC1774446
- DOI: 10.1136/gut.2004.047696
Relationship between symptoms and disordered continence mechanisms in women with idiopathic faecal incontinence
Abstract
Background and aims: Anal sphincter weakness and rectal sensory disturbances contribute to faecal incontinence (FI). Our aims were to investigate the relationship between symptoms, risk factors, and disordered anorectal and pelvic floor functions in FI.
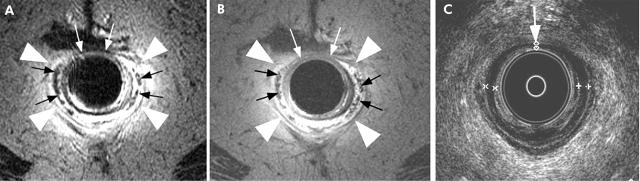
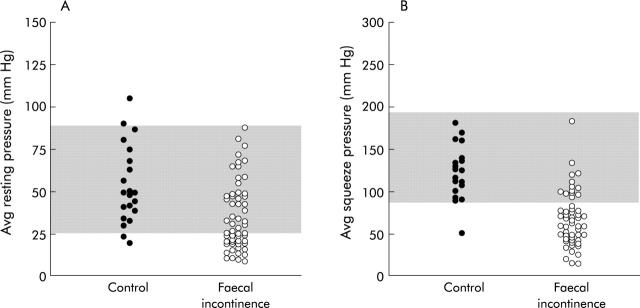
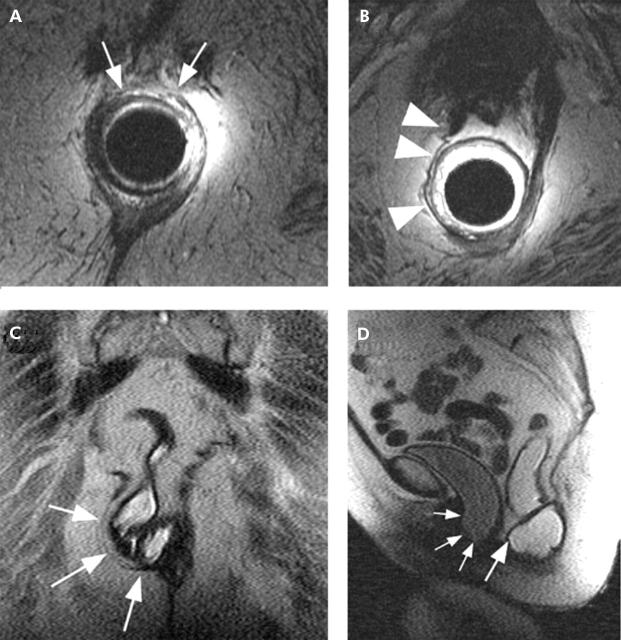
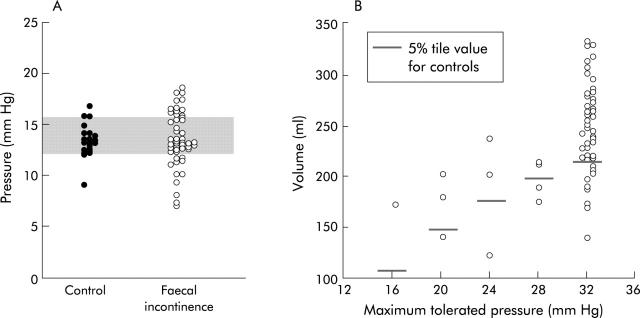
Methods: In 52 women with "idiopathic" FI and 21 age matched asymptomatic women, we assessed symptoms by standardised questionnaire, anal pressures by manometry, anal sphincter appearance by endoanal ultrasound and magnetic resonance imaging (MRI), pelvic floor motion by dynamic MRI, and rectal compliance and sensation by a barostat.
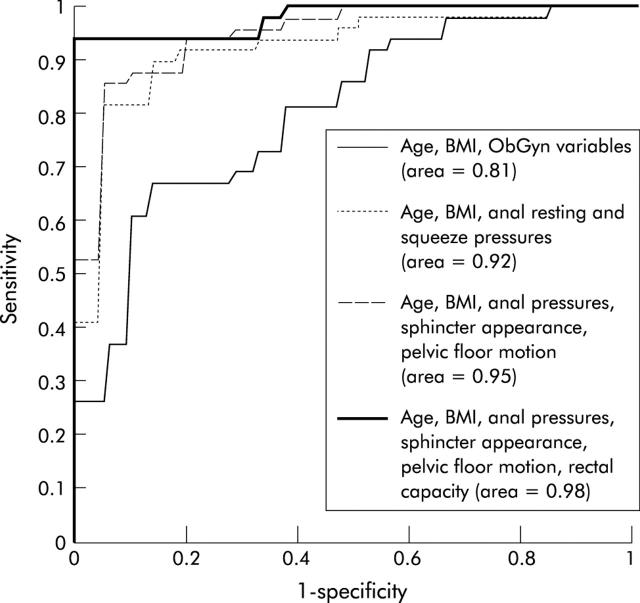
Results: The prevalence of anal sphincter injury (by imaging), reduced anal resting pressure (35% of FI), and reduced squeeze pressures (73% of FI) was higher in FI compared with controls. Puborectalis atrophy (by MRI) was associated (p<0.05) with FI and with impaired anorectal motion during pelvic floor contraction. Volume and pressure thresholds for the desire to defecate were lower, indicating rectal hypersensitivity, in FI. The rectal volume at maximum tolerated pressure (that is, rectal capacity) was reduced in 25% of FI; this volume was associated with the symptom of urge FI (p<0.01) and rectal hypersensitivity (p = 0.02). A combination of predictors (age, body mass index, symptoms, obstetric history, and anal sphincter appearance) explained a substantial proportion of the interindividual variation in anal squeeze pressure (45%) and rectal capacity (35%).
Conclusions: Idiopathic FI in women is a multifactorial disorder resulting from one or more of the following: a disordered pelvic barrier (anal sphincters and puborectalis), or rectal capacity or sensation.
Figures

References
-
- Drossman DA, Li Z, Andruzzi E, et al. U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci 1993;38:1569–80. - PubMed
-
- Nelson R, Norton N, Cautley E, et al. Community-based prevalence of anal incontinence. JAMA 1995;274:559–61. - PubMed
-
- Reilly W, Talley N, Pemberton J. Fecal incontinence: prevalence and risk factors in the community. Gastroenterology 1995;108:A32.
-
- Sultan AH, Kamm MA. Faecal incontinence after childbirth. Br J Obstet Gynaecol 1997;104:979–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources