

Long-term follow-up after complete ablation of Barrett's esophagus with argon plasma coagulation
- PMID: 15754401
- PMCID: PMC4250710
- DOI: 10.3748/wjg.v11.i8.1182
Long-term follow-up after complete ablation of Barrett's esophagus with argon plasma coagulation
Abstract
Aim: To report the long-term outcome of patients after complete ablation of non-neoplastic Barrett's esophagus (BE) with respect to BE relapse and development of intraepithelial neoplasia or esophageal adenocarcinoma.
Methods: In 70 patients with histologically proven non-neoplastic BE, complete BE ablation was achieved by argon plasma coagulation (APC) and high-dose proton pump inhibitor therapy (120 mg omeprazole daily). Sixty-six patients (94.4%) underwent further surveillance endoscopy. At each surveillance endoscopy four-quadrant biopsies were taken from the neo-squamous epithelium at 2 cm intervals depending on the pre-treatment length of BE mucosa beginning at the neo-Z-line, and from any endoscopically suspicious lesion.
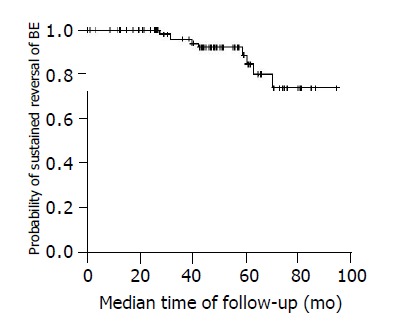
Results: The median follow-up of 66 patients was 51 mo (range 9-85 mo) giving a total of 280.5 patient years. A mean of 6 biopsies were taken during surveillance endoscopies. In 13 patients (19.7%) tongues or islands suspicious for BE were found during endoscopy. In 8 of these patients (12.1%) non-neoplastic BE relapse was confirmed histologically giving a histological relapse rate of 3% per year. In none of the patients, intraepithelial neoplasia nor an esophageal adenocarcinoma was detected. Logistic regression analysis identified endoscopic detection of islands or tongues as the only positive predictor of BE relapse (P = 0.0004).
Conclusion: The long-term relapse rate of non-neoplastic BE following complete ablation with high-power APC is low (3% per year).
Figures
Similar articles
-
Ablation of residual Barrett's epithelium after endoscopic resection: a randomized long-term follow-up study of argon plasma coagulation vs. surveillance (APE study).Endoscopy. 2014 Jan;46(1):6-12. doi: 10.1055/s-0033-1358813. Epub 2013 Dec 18. Endoscopy. 2014. PMID: 24353120 Clinical Trial.
-
Endoscopic ablation of Barrett's esophagus using high power setting argon plasma coagulation: a prospective study.World J Gastroenterol. 2005 Mar 28;11(12):1872-5. doi: 10.3748/wjg.v11.i12.1872. World J Gastroenterol. 2005. PMID: 15793884 Free PMC article. Clinical Trial.
-
Long-term follow-up and factors predictive of recurrence in Barrett's esophagus treated by argon plasma coagulation and acid suppression.Endoscopy. 2002 Dec;34(12):950-5. doi: 10.1055/s-2002-35847. Endoscopy. 2002. PMID: 12471537 Clinical Trial.
-
Diagnosis and Management of Low-Grade Dysplasia in Barrett's Esophagus: Expert Review From the Clinical Practice Updates Committee of the American Gastroenterological Association.Gastroenterology. 2016 Nov;151(5):822-835. doi: 10.1053/j.gastro.2016.09.040. Epub 2016 Oct 1. Gastroenterology. 2016. PMID: 27702561 Review.
-
Barrett's esophagus: current and future management.Compr Ther. 1994;20(1):36-43. Compr Ther. 1994. PMID: 8137618 Review.
Cited by
-
The treatments and postoperative complications of esophageal cancer: a review.J Cardiothorac Surg. 2020 Jul 6;15(1):163. doi: 10.1186/s13019-020-01202-2. J Cardiothorac Surg. 2020. PMID: 32631428 Free PMC article.
-
Diode laser treatment of Barrett's esophagus: long-term results.Lasers Med Sci. 2011 Mar;26(2):223-8. doi: 10.1007/s10103-010-0836-3. Epub 2010 Sep 7. Lasers Med Sci. 2011. PMID: 20821340
-
BOB CAT: A Large-Scale Review and Delphi Consensus for Management of Barrett's Esophagus With No Dysplasia, Indefinite for, or Low-Grade Dysplasia.Am J Gastroenterol. 2015 May;110(5):662-82; quiz 683. doi: 10.1038/ajg.2015.55. Epub 2015 Apr 14. Am J Gastroenterol. 2015. PMID: 25869390 Free PMC article. Review.
-
The evolution of endoscopic therapy for Barrett's esophagus.Ther Adv Gastrointest Endosc. 2021 Oct 22;14:26317745211051834. doi: 10.1177/26317745211051834. eCollection 2021 Jan-Dec. Ther Adv Gastrointest Endosc. 2021. PMID: 34708204 Free PMC article. Review.
-
Prospective randomized trial of argon plasma coagulation ablation versus endoscopic surveillance of Barrett's esophagus in patients treated with antisecretory medication.Dig Dis Sci. 2009 Dec;54(12):2606-11. doi: 10.1007/s10620-008-0662-7. Dig Dis Sci. 2009. PMID: 19101798 Clinical Trial.
References
-
- Falk GW. Barrett's esophagus. Gastroenterology. 2002;122:1569–1591. - PubMed
-
- Haag S, Holtmann G. Reflux disease and Barrett's esophagus. Endoscopy. 2003;35:112–117. - PubMed
-
- Spechler SJ, Goyal RK. Barrett's esophagus. N Engl J Med. 1986;315:362–371. - PubMed
-
- Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett's esophagus in asymptomatic individuals. Gastroenterology. 2002;123:461–467. - PubMed
-
- Hameeteman W, Tytgat GN, Houthoff HJ, van den Tweel JG. Barrett's esophagus: development of dysplasia and adenocarcinoma. Gastroenterology. 1989;96:1249–1256. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
