

Increased capsaicin receptor TRPV1 in skin nerve fibres and related vanilloid receptors TRPV3 and TRPV4 in keratinocytes in human breast pain
- PMID: 15755319
- PMCID: PMC554997
- DOI: 10.1186/1472-6874-5-2
Increased capsaicin receptor TRPV1 in skin nerve fibres and related vanilloid receptors TRPV3 and TRPV4 in keratinocytes in human breast pain
Abstract
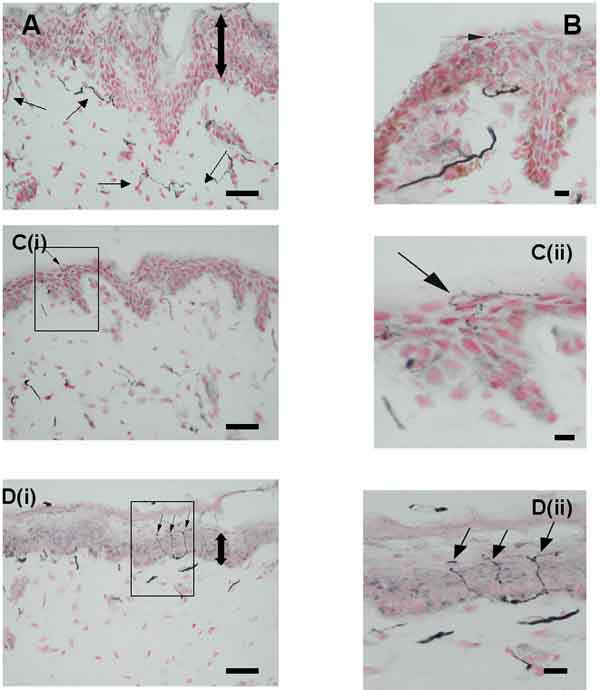
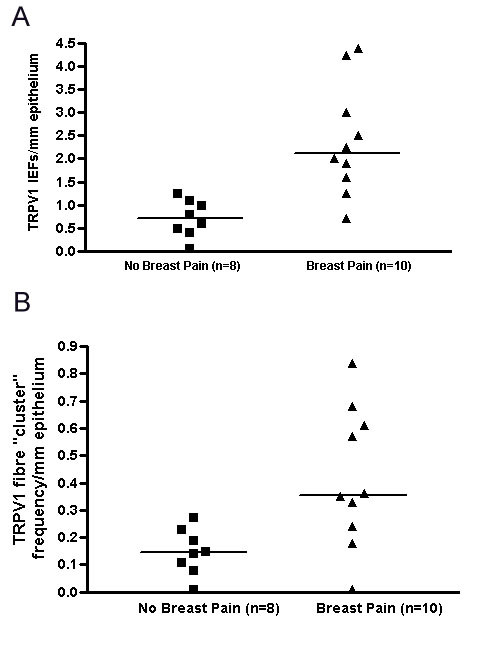
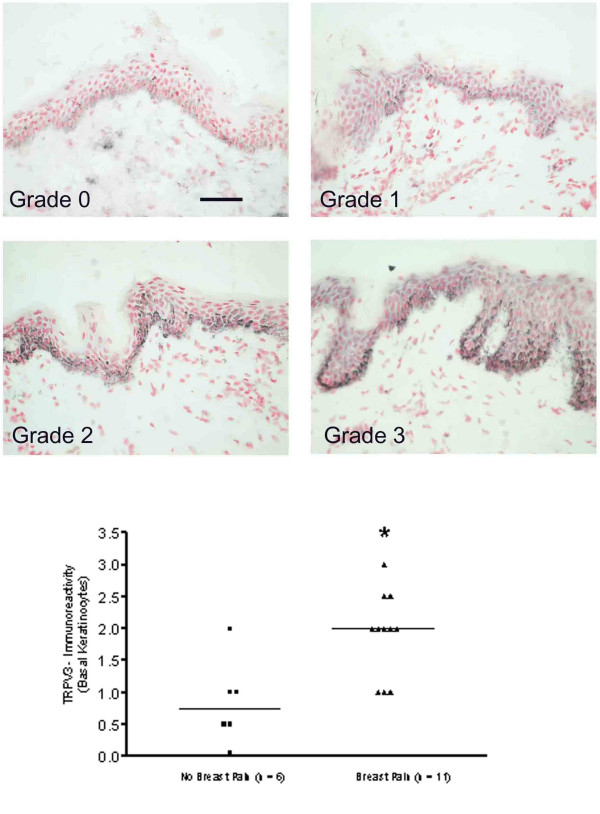
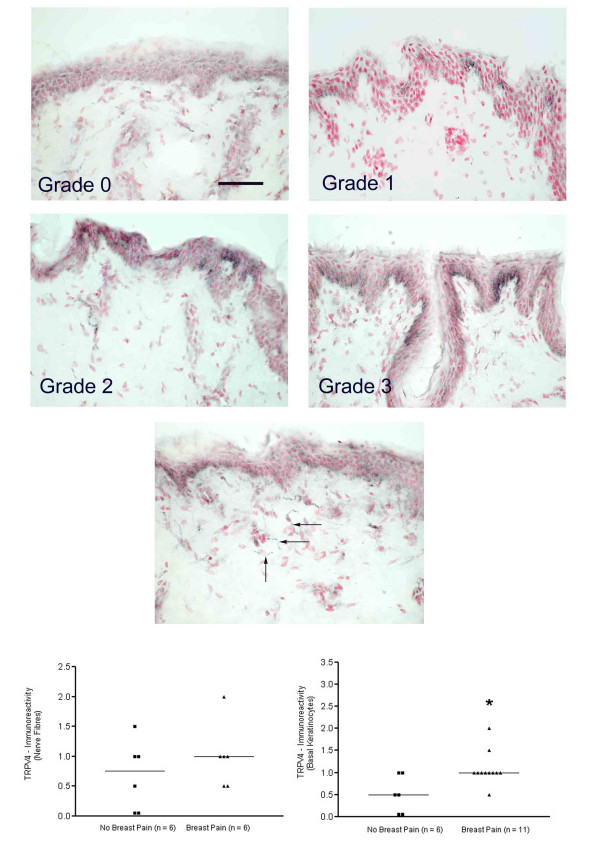
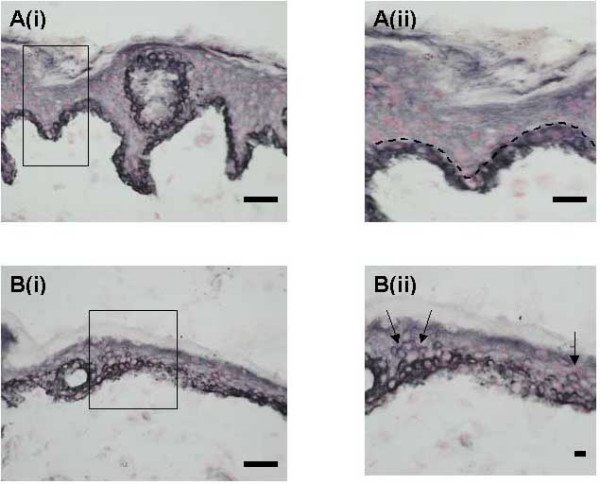
BACKGROUND: Breast pain and tenderness affects 70% of women at some time. These symptoms have been attributed to stretching of the nerves with increase in breast size, but tissue mechanisms are poorly understood. METHODS: Eighteen patients (n = 12 breast reduction and n = 6 breast reconstruction) were recruited and assessed for breast pain by clinical questionnaire. Breast skin biopsies from each patient were examined using immunohistological methods with specific antibodies to the capsaicin receptor TRPV1, related vanilloid thermoreceptors TRPV3 and TRPV4, and nerve growth factor (NGF). RESULTS: TRPV1-positive intra-epidermal nerve fibres were significantly increased in patients with breast pain and tenderness (TRPV1 fibres / mm epidermis, median [range] - no pain group, n = 8, 0.69 [0-1.27]; pain group, n = 10, 2.15 [0.77-4.38]; p = 0.0009). Nerve Growth Factor, which up-regulates TRPV1 and induces nerve sprouting, was present basal keratinocytes: some breast pain specimens also showed NGF staining in supra-basal keratinocytes. TRPV4-immunoreactive fibres were present in sub-epidermis but not significantly changed in painful breast tissue. Both TRPV3 and TRPV4 were significantly increased in keratinocytes in breast pain tissues; TRPV3, median [range] - no pain group, n = 6, 0.75 [0-2]; pain group, n = 11, 2 123, p = 0.008; TRPV4, median [range] - no pain group, n = 6, [0-1]; pain group, n = 11, 1 [0.5-2], p = 0.014). CONCLUSION: Increased TRPV1 intra-epidermal nerve fibres could represent collateral sprouts, or re-innervation following nerve stretch and damage by polymodal nociceptors. Selective TRPV1-blockers may provide new therapy in breast pain. The role of TRPV3 and TRPV4 changes in keratinocytes deserve further study.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
