

Reversible MR imaging abnormalities following cerebral venous thrombosis
- PMID: 15760874
- PMCID: PMC7976480
Reversible MR imaging abnormalities following cerebral venous thrombosis
Abstract
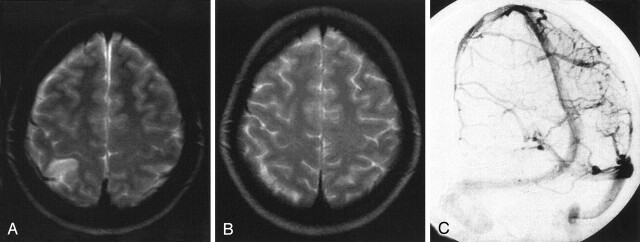
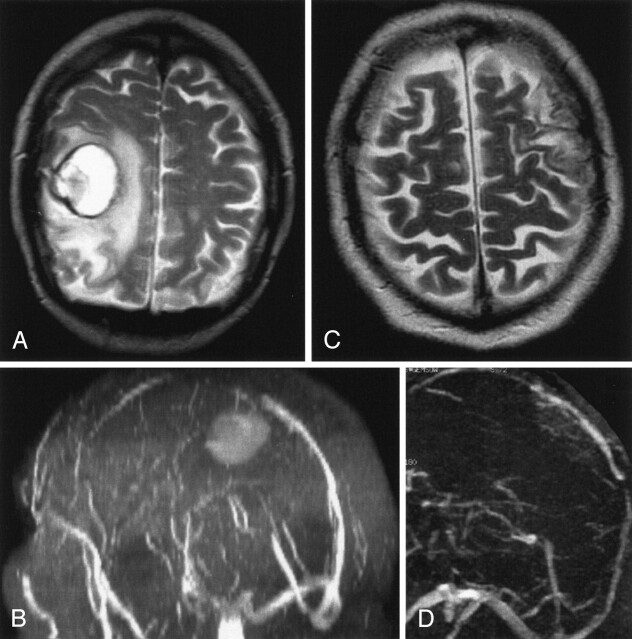
Background and purpose: Although rare, cerebral venous thrombosis (CVT) is being diagnosed more frequently owing to improved imaging techniques. The venous infarcts caused by CVT in 50% of patients are largely reversible and differ from arterial stroke. Our purpose was to study the time-dependent changes of venous infarcts on MR images and to define the variables that influence lesion volume in humans.
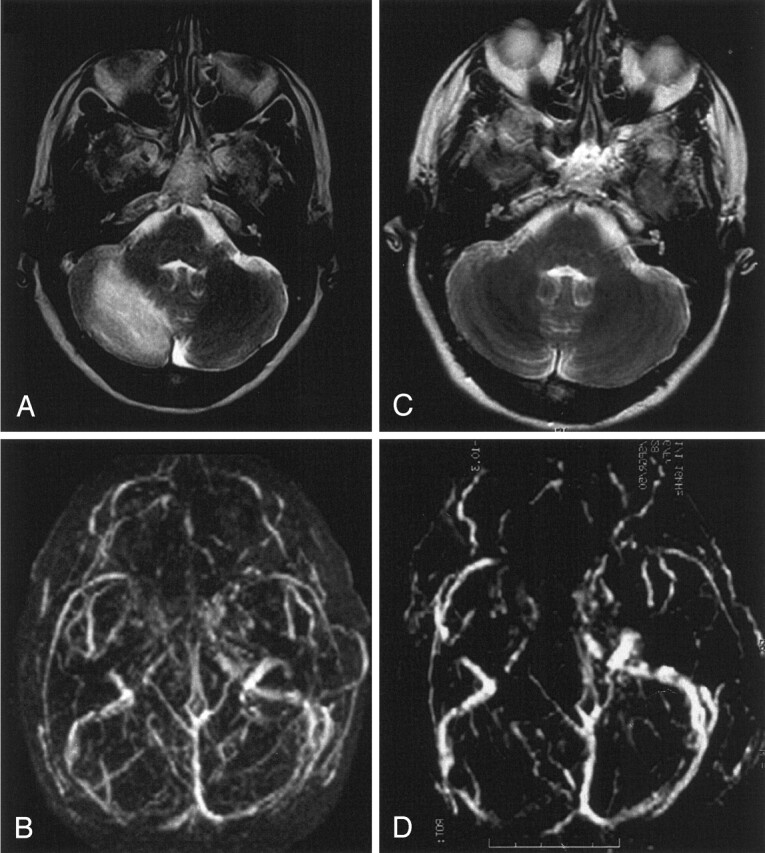
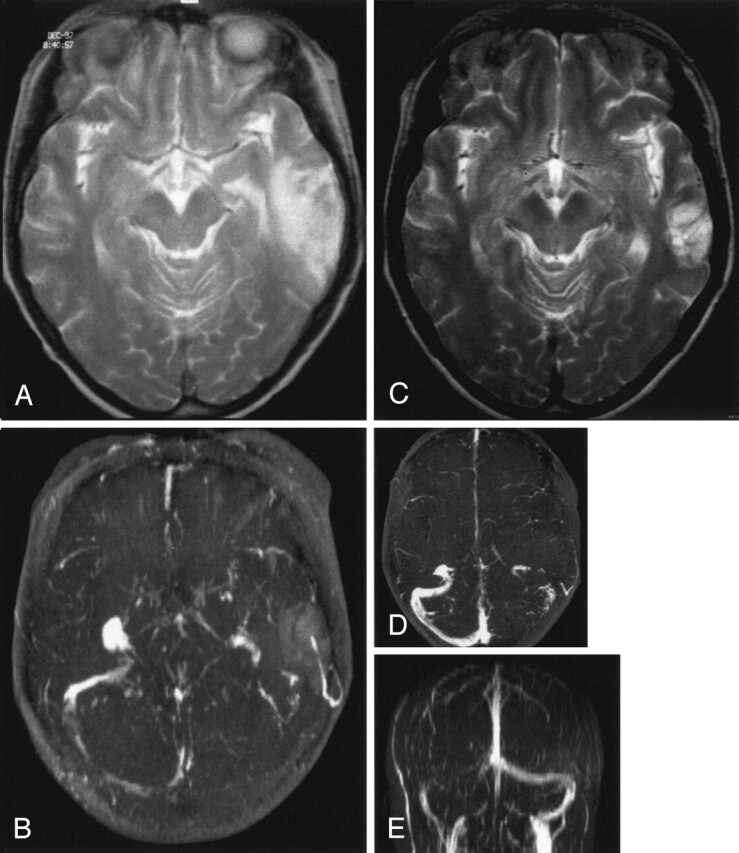
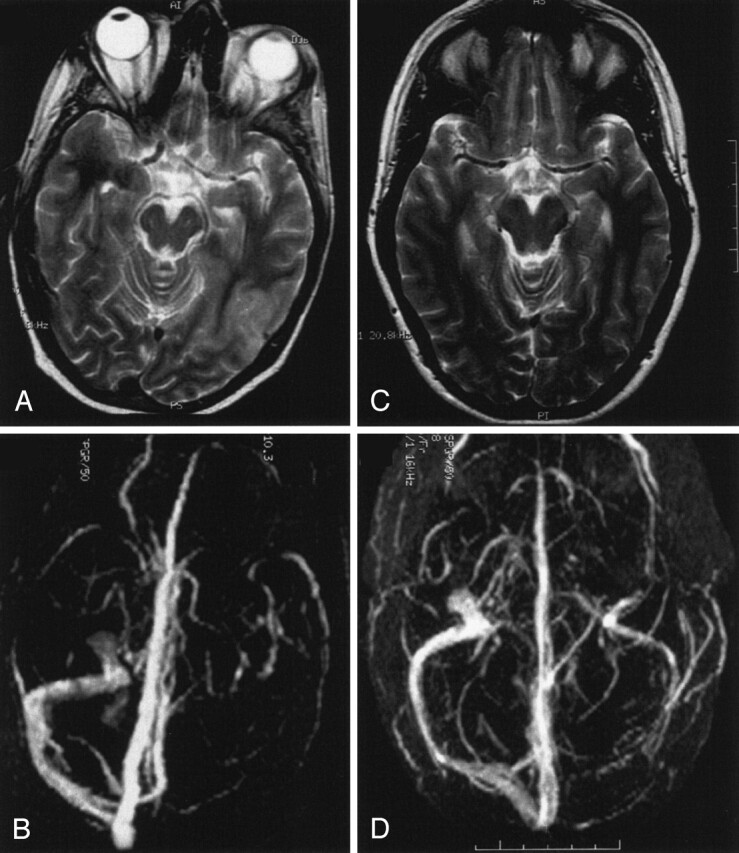
Methods: MR images and venous angiograms were evaluated in 15 consecutive patients with venous infarcts due to CVT of sinus, cortical, or internal veins. All patients were treated with intravenous dose-adjusted heparin followed by oral anticoagulation for 12 months. Reduction of signal intensity changes on T1- and T2-weighted images was correlated to the degree of recanalization, age, initial absolute lesion size, and hemorrhage.
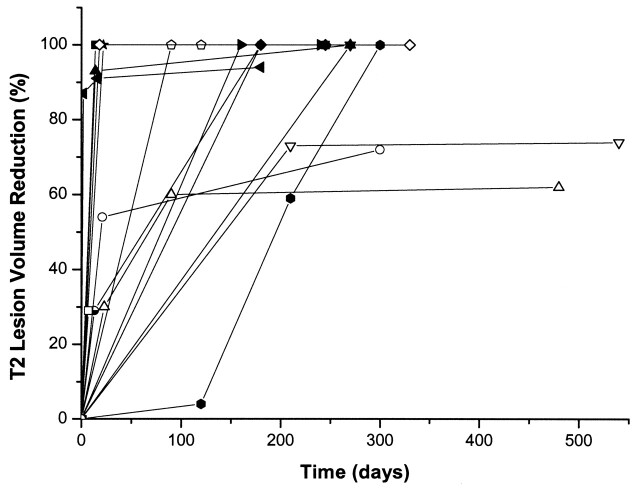
Results: Within the first 30 days, we found a significant correlation between the volume of the lesion on T1-weighted images and recanalization. However, early recanalization did not influence the final lesion volume after 12 months. Eleven patients showed complete resolution of changes on T1- and T2-weighted images. Age of the patients influenced initial absolute volume of brain damage.
Conclusion: In venous stroke, even large parenchymal changes can resolve completely independent from recanalization of the thrombosed veins and sinuses. A plausible hypothesis is that venous infarcts largely consist of a persistent edema and that the lesion volume is influenced by the development of collateral veins. However, further investigations are necessary to understand the underlying abnormal mechanisms.
Figures
References
-
- Nakase H, Heimann A, Kempski O. Alterations of regional cerebral blood flow and oxygen saturation in a rat sinus-vein thrombosis model. Stroke 1996;27:720–727 - PubMed
-
- Röther J, Waggie K, van Bruggen N, de Crespigny AJ, Moseley ME. Experimental cerebral venous thrombosis: evaluation using magnetic resonance imaging. J Cereb Blood Flow Metab 1996;16:1353–1361 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical