

Case Reports
Cortical involvement in Marchiafava-Bignami disease
Affiliations
- PMID: 15760886
- PMCID: PMC7976492
Item in Clipboard
Case Reports
Cortical involvement in Marchiafava-Bignami disease
AJNR Am J Neuroradiol.
2005 Mar.
Abstract
Marchiafava-Bignami disease (MBD), a rare complication of chronic alcoholism, is characterized by primary demyelination of the corpus callosum. We report two cases of MBD in which fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted imaging studies revealed symmetrical hyperintense lesions in the cerebral cortex (particularly in the lateral-frontal regions) in addition to the callosal lesions, which suggests an association of diffuse cortical lesions such as Morel's laminar sclerosis with MBD.
Figures

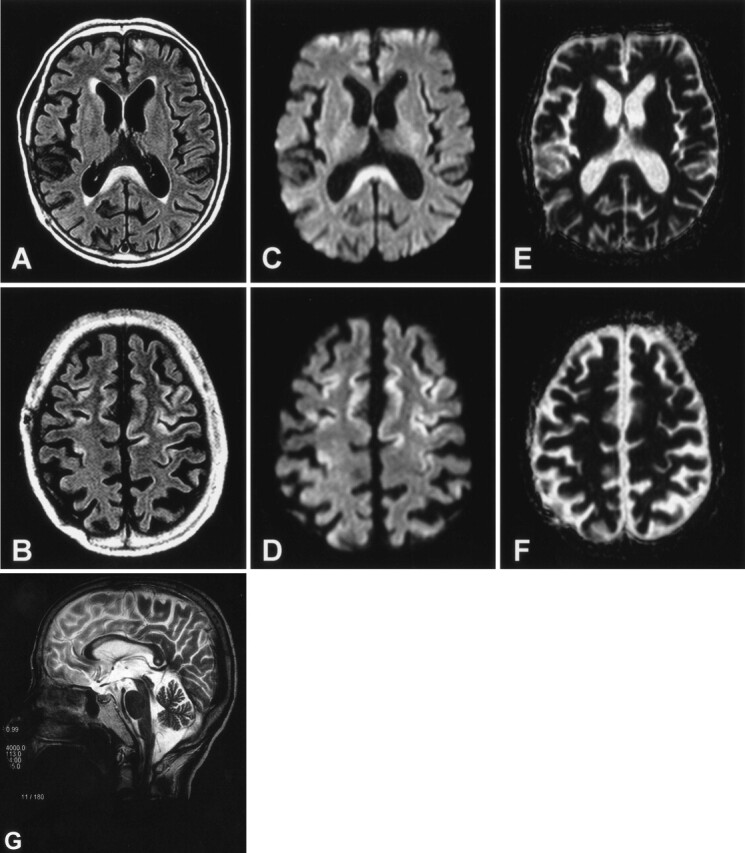
MR images in patient 1. Axial FLAIR images on admission show hyperintensity in the corpus callosum (A) and the cerebral cortex (B). Diffusion-weighted images (C and D) also show hyperintensity in these regions with relatively decreased ADC values (see Fig 3). The decreased ADC values, however, are inconspicuous on ADC mapping (E and F). Follow-up T2-weighted sagittal image obtained 10 days after the initial study shows callosal lesions mainly involving the central part of the splenium and body (G).
MR images in patient 2. Axial FLAIR images on admission show hyperintensity in the corpus callosum (A) and the cerebral cortex (B). Diffusion-weighted images (C and D) also show hyperintensity in these regions with relatively decreased ADC values (see Fig 3). The decreased ADC values, however, are inconspicuous on ADC mapping (E and F). Follow-up T2-weighted sagittal image obtained 10 days after the initial study shows callosal lesions mainly involving the central part of the splenium and body (G).

Comparison of signal intensities on diffusion-weighted images with ADC values on ADC maps. Each coordinate of regions of interest in the ADC maps is the same as that in diffusion-weighted images. ADC values are reduced in regions with high signal intensity on diffusion-weighted images (regions 3 and 4 in each patient). Asterisks denote regions in affected cortex identified by high signal intensity on diffusion-weighted images.
References
-
- Koeppen AH, Barron KD. Marchiafava-Bignami disease. Neurology 1978;28:290–294 - PubMed
-
- Ruiz-Martínez J, Martínez Pérez-Balsa A, Ruibal M, et al. Marchiafava-Bignami disease with widespread extracallosal lesions and favourable course. Neuroradiology 1999;41:40–43 - PubMed
-
- Harper C, Butterworth R. Nutritional and metabolic disorders. In: Graham DI, Lantos PL, eds. Greenfield’s Neuropathology. 6th ed. London: Arnold,1997. :616–617
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical