

New aspects of the ventricular septum and its function: an echocardiographic study
- PMID: 15761045
- PMCID: PMC1769152
- DOI: 10.1136/hrt.2004.043422
New aspects of the ventricular septum and its function: an echocardiographic study
Abstract
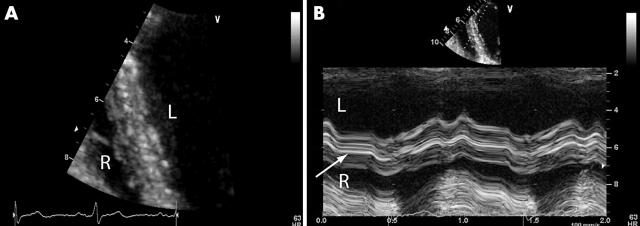
Objectives: To examine whether the line dividing the septum into two layers is found consistently by conventional echocardiography and to evaluate functional differences in the right and left side of the septum in terms of wall thickening, strain rate, and strain imaging.
Design: In a systematic study in 30 normal subjects, M mode and Doppler myocardial imaging data from the interventricular septum (IVS) were recorded. Velocity curves, regional strain rate, and strain profiles were obtained. Systolic deformation (wall thickening, radial and longitudinal strain rate, and strain) of both sides were assessed. Furthermore, three patients with one sided abnormalities were studied.
Results: A bright echo consistently segmented the IVS into a left and right part. In this normal population radial deformation was different for the left and right side of the septum (mean (SD) wall thickening on the left, 49 (46)%, and on the right, 17 (38)%; strain rate on the left, 3.8 (0.6) 1/s, and on the right, 2.1 (1.9) 1/s; strain on the left, 41 (17)%, and on the right, 22 (14)%), whereas longitudinal deformation was found to be similar (strain rate on the left, -2.2 (0.7) 1/s, and on the right, -2.0 (0.6) 1/s; strain on the left, -28 (12)%, and on the right, -25 (12)%). The presented clinical examples show that abnormalities can be strictly limited to one layer.
Conclusions: Differential radial deformation and knowledge of fibre architecture showing an abrupt change in the middle of the septum, together with the clinical cases, suggest the septum to be a morphologically and functionally bilayered structure potentially supplied by different coronary arteries.
Figures







Comment in
-
The interventricular septum is functionally bilayered: a fresh look at a well known structure.Heart. 2005 Oct;91(10):1260-1. doi: 10.1136/hrt.2004.057646. Heart. 2005. PMID: 16162607 Free PMC article.
References
-
- Feigenbaum H. Echocardiography. 3rd ed. Philadelphia: Lea and Febiger, 1981:454.
-
- Feneley MP, Gavaghan TP, Baron DW, et al. Contribution of left ventricular contraction to the generation of right ventricular systolic pressure in the human heart. Circulation 1985;71:473–80. - PubMed
-
- Santamore WP, Constantinescu M, Minczak BM, et al. Contribution of each ventricular wall to ventricular interdependence. Basic Res Cardiol 1988;83:424–30. - PubMed
-
- Brinker JA, Weiss JL, Lappe DL, et al. Leftward septal displacement during right ventricular loading in man. Circulation 1980;61:626–33. - PubMed
-
- Santamore WP, Lynch PR, Heckman JL, et al. Left ventricular effects on right ventricular developed pressure. J Appl Physiol 1976;41:925–30. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources