

Combined intra-extracanal approach to lumbosacral disc herniations with bi-radicular involvement. Technical considerations from a surgical series of 15 cases
- PMID: 15761707
- PMCID: PMC3489333
- DOI: 10.1007/s00586-004-0862-6
Combined intra-extracanal approach to lumbosacral disc herniations with bi-radicular involvement. Technical considerations from a surgical series of 15 cases
Abstract
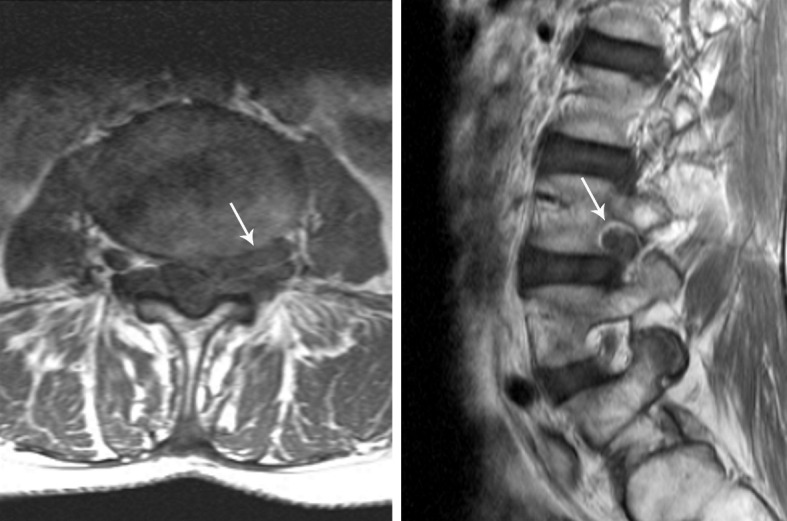
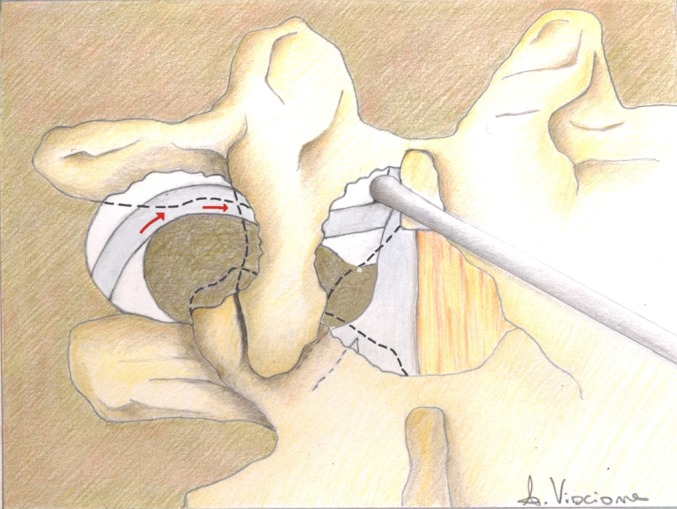
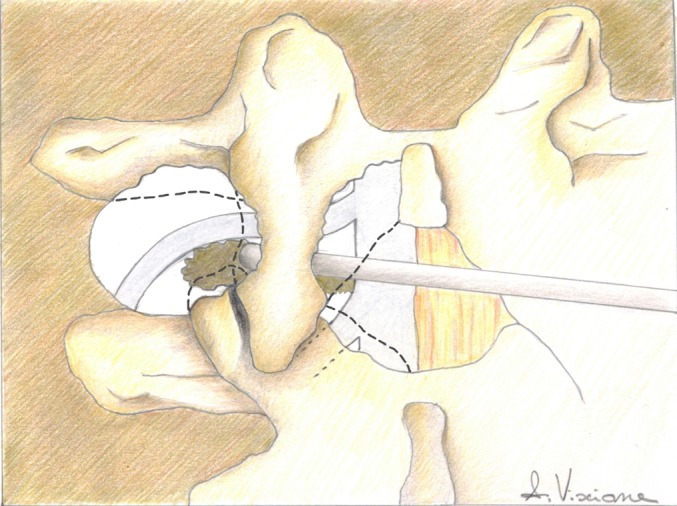
Large lumbosacral disc herniations effacing both the paramedian and the foraminal area often cause double radicular compression. Surgical management of these lesions may be difficult. A traditional interlaminar approach usually brings into view only the paramedian portion of the intervertebral disc, unless the lateral bone removal is considerably increased. Conversely, the numerous far-lateral approaches proposed for removing foraminal or extraforaminal disc herniations would decompress the exiting nerve root only. Overall, these approaches share the drawback of controlling the neuroforamen on one side alone. A combined intra-extraforaminal exposure is a useful yet rarely reported approach. Over a 3-year period, 15 patients with bi-radicular symptoms due to large disc herniations of the lumbar spine underwent surgery through a combined intra-extracanal approach. A standard medial exposure with an almost complete hemilaminectomy of the upper vertebra was combined with an extraforaminal exposure, achieved by minimal drilling of the inferior facet joint, the lateral border of the pars interarticularis and the inferior margin of the superior transverse process. The herniated discs were removed using key maneuvers made feasible by working simultaneously on both operative windows. In all cases the disc herniation could be completely removed, thus decompressing both nerve roots. Radicular pain was fully relieved without procedure-related morbidity. The intra-extraforaminal exposure was particularly useful in identifying the extraforaminal nerve root early. Early identification was especially advantageous when periradicular scar tissue hid the nerve root from view, as it did in patients who had undergone previous surgery at the same site or had long-standing radicular symptoms. Controlling the foramen on both sides also reduced the risk of leaving residual disc fragments. A curved probe was used to push the disc material outside the foramen. In conclusion, specific surgical maneuvers made feasible by a simultaneous extraspinal and intraspinal exposure allow quick, safe and complete removal of lumbosacral disc herniations with paramedian and foraminal extension.
Figures
Similar articles
-
A minimally invasive transmuscular approach to far-lateral L5-S1 level disc herniations: a prospective study.J Spinal Disord Tech. 2007 Apr;20(2):132-8. doi: 10.1097/01.bsd.0000211268.43744.2a. J Spinal Disord Tech. 2007. PMID: 17414982 Clinical Trial.
-
Transmuscular trocar technique - minimal access spine surgery for far lateral lumbar disc herniations.Minim Invasive Neurosurg. 2007 Oct;50(5):304-7. doi: 10.1055/s-2007-990292. Minim Invasive Neurosurg. 2007. PMID: 18058649
-
Percutaneous endoscopic discectomy for far lateral lumbar disc herniations: prospective study and outcome of 66 patients.Minim Invasive Neurosurg. 2007 Apr;50(2):91-7. doi: 10.1055/s-2007-984383. Minim Invasive Neurosurg. 2007. PMID: 17674295
-
Minimally invasive far lateral microendoscopic discectomy for extraforaminal disc herniation at the lumbosacral junction: cadaveric dissection and technical case report.Spine J. 2007 Jul-Aug;7(4):414-21. doi: 10.1016/j.spinee.2006.07.008. Epub 2007 Jan 30. Spine J. 2007. PMID: 17630139 Review.
-
Foraminal and far lateral lumbar disc herniations: surgical alternatives and outcome measures.Spinal Cord. 2002 Oct;40(10):491-500. doi: 10.1038/sj.sc.3101319. Spinal Cord. 2002. PMID: 12235530 Review.
Cited by
-
Management of disc herniations with bi-radicular symptoms via combined lateral and interlaminar approach.Neurosurg Rev. 2010 Jan;33(1):97-105. doi: 10.1007/s10143-009-0218-0. Neurosurg Rev. 2010. PMID: 19688231
-
A survey of the "surgical and research" articles in the European Spine Journal, 2006.Eur Spine J. 2007 Jan;16(1):11-8. doi: 10.1007/s00586-006-0273-y. Epub 2006 Dec 8. Eur Spine J. 2007. PMID: 17160392 Free PMC article. Review. No abstract available.
-
Transforaminal lumbar interbody fusion using one diagonal fusion cage with unilateral pedicle screw fixation for treatment of massive lumbar disc herniation.Indian J Orthop. 2016 Sep;50(5):473-478. doi: 10.4103/0019-5413.189595. Indian J Orthop. 2016. PMID: 27746488 Free PMC article.
-
Hidden blood loss in percutaneous endoscopic lumbar discectomy via the posterolateral approach.Jt Dis Relat Surg. 2025 Jan 2;36(1):56-64. doi: 10.52312/jdrs.2025.2065. Epub 2024 Dec 18. Jt Dis Relat Surg. 2025. PMID: 39719902 Free PMC article.
-
Combined Interlaminar and Paraisthmic Approach for Co-existing Intracanal and Foraminal Lesion.Korean J Spine. 2015 Dec;12(4):256-60. doi: 10.14245/kjs.2015.12.4.256. Epub 2015 Dec 31. Korean J Spine. 2015. PMID: 26834813 Free PMC article.
References
-
- Lorenzo N, Porta F, Onnis G, Cannas A, Arbau G, Maleci A. Pars interarticularis fenestration in the treatment of foraminal lumbar disc herniation: a further surgical approach. Neurosurgery. 1998;42:87–89. - PubMed
-
- Donaldson WF, Star MJ, Thorne RP. Surgical treatment for the far lateral herniated lumbar disc. Spine. 1993;18:1263–1267. - PubMed
-
- Ebeling U, Kalbarcyk H, Reulen HJ. Microsurgical reoperation following lumbar disc surgery. Timing, surgical findings, and outcome in 92 patients. J Neurosurg. 1989;70:397–404. - PubMed
-
- Epstein NE. Evaluation of varied surgical approaches used in the management of 170 far-lateral lumbar disc herniations: indications and results. J Neurosurg. 1995;83:648–656. - PubMed
-
- Epstein NE. Foraminal and far lateral lumbar disc herniations: surgical alternatives and outcome measures. Spinal Cord. 2002;40:491–500. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
