

Assessment of CD8 T cell immune activation markers to monitor response to antiretroviral therapy among HIV-1 infected patients in Côte d'Ivoire
- PMID: 15762885
- PMCID: PMC1809342
- DOI: 10.1111/j.1365-2249.2005.02734.x
Assessment of CD8 T cell immune activation markers to monitor response to antiretroviral therapy among HIV-1 infected patients in Côte d'Ivoire
Abstract
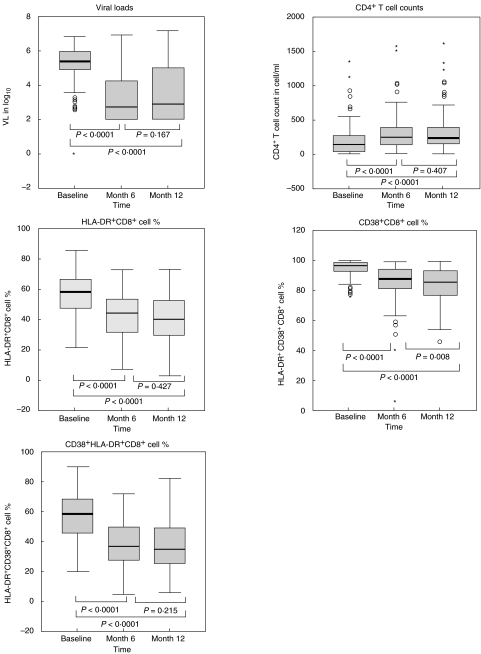
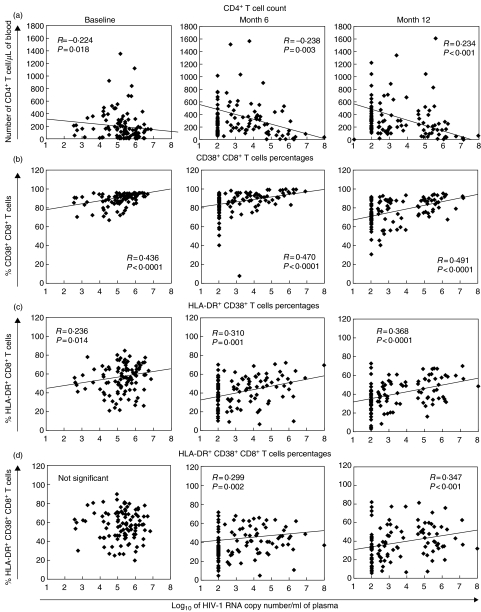
Because of the paucity of plasma HIV RNA viral load (VL) tests in resource-poor settings, the CD4(+) T cell count is often used as the sole laboratory marker to evaluate the effectiveness of antiretroviral therapy (ART) in HIV-infected patients. In untreated patients, the level of activated T cells is positively correlated with VL and represents a prognostic marker of HIV infection. However, little is known about its value to predict early drug failure, taking into account the relatively high non-specific immune activation background observed in many resource-limited tropical countries. We assessed the use of immune activation markers (expression of CD38 and/or human leucocyte antigen-DR on CD8(+) lymphocytes) to predict virological response to ART in a cohort of HIV-1 infected patients in Abidjan, Côte d'Ivoire. Correlations between VL, absolute CD4(+) T cell counts and immune activation levels were examined in 111 HIV patient samples at baseline and after 6 and 12 months of therapy. The percentage of CD38(+) CD8(+) T cells appeared to be the best correlate of VL. In contrast, changes in CD4(+) T cell counts provided a poor correlate of virological response to ART. Unfortunately, CD38(+) CD8(+) percentages lacked specificity for the determination of early virological drug failure and did not appear to be reliable surrogates of RNA viral load. CD38(+) CD8(+) T cell percentages may, rather, provide a sensitive estimate of the overall immune recovery, and be a useful extra laboratory parameter to CD4 counts that would contribute to improve the clinical management of HIV-infected people when VL testing facilities are lacking.
Figures

Similar articles
-
Changes in levels of immune activation and reconstitution markers among HIV-1-infected Africans receiving antiretroviral therapy.AIDS. 2003 Jul;17 Suppl 3:S17-22. doi: 10.1097/00002030-200317003-00003. AIDS. 2003. PMID: 14565605
-
HIV-1-specific cytolytic T-lymphocyte activity correlates with lower viral load, higher CD4 count, and CD8+CD38-DR- phenotype: comparison of statistical methods for measurement.J Acquir Immune Defic Syndr. 1999 Sep 1;22(1):19-30. doi: 10.1097/00042560-199909010-00003. J Acquir Immune Defic Syndr. 1999. PMID: 10534143
-
Changes in levels of T cell subpopulations to monitor the response to antiretroviral therapy among HIV-1-infected patients during two years of HIV-1 replication suppression.Scand J Infect Dis. 2013 May;45(5):368-77. doi: 10.3109/00365548.2012.744465. Epub 2012 Nov 28. Scand J Infect Dis. 2013. PMID: 23186319
-
Association of CD8+ T lymphocyte subsets with the most commonly used markers to monitor HIV type 1 infection in children treated with highly active antiretroviral therapy.AIDS Res Hum Retroviruses. 2001 Apr 10;17(6):525-32. doi: 10.1089/08892220151126607. AIDS Res Hum Retroviruses. 2001. PMID: 11350666
-
Impact of CD8+ T-cell activation on CD4+ T-cell recovery and mortality in HIV-infected Ugandans initiating antiretroviral therapy.AIDS. 2011 Nov 13;25(17):2123-31. doi: 10.1097/QAD.0b013e32834c4ac1. AIDS. 2011. PMID: 21881481 Free PMC article.
Cited by
-
Utilization of immunological ratios in HIV: Implications for monitoring and therapeutic strategies.Medicine (Baltimore). 2024 Mar 1;103(9):e37354. doi: 10.1097/MD.0000000000037354. Medicine (Baltimore). 2024. PMID: 38428854 Free PMC article.
-
Elevated CD8 counts during HAART are associated with HIV virologic treatment failure.J Acquir Immune Defic Syndr. 2011 Aug 15;57(5):396-403. doi: 10.1097/QAI.0b013e318221c62a. J Acquir Immune Defic Syndr. 2011. PMID: 21602694 Free PMC article.
-
Advanced in immunological monitoring of HIV infection: profile of immune cells and cytokines in people living with HIV-1 in Benin.BMC Immunol. 2024 Apr 20;25(1):22. doi: 10.1186/s12865-024-00615-1. BMC Immunol. 2024. PMID: 38643073 Free PMC article.
-
The role of CD38 in HIV infection.AIDS Res Ther. 2021 Apr 5;18(1):11. doi: 10.1186/s12981-021-00330-6. AIDS Res Ther. 2021. PMID: 33820568 Free PMC article. Review.
-
Early changes in T-cell activation predict antiretroviral success in salvage therapy of HIV infection.J Acquir Immune Defic Syndr. 2008 Jun 1;48(2):149-55. doi: 10.1097/QAI.0b013e31816d9c3b. J Acquir Immune Defic Syndr. 2008. PMID: 18360289 Free PMC article.
References
-
- Mellors JW, Kingsley LA, Rinaldo CR, et al. Quantitation of HIV-1 RNA in plasma predicts the outcome after seroconversion. Ann Intern Med. 1995;122:573–9. - PubMed
-
- Cao YC, Qin L, Zhang L, et al. Virologic and immunologic characterisation of longterm survivors of human immunodeficiency virus type 1 infection. N Engl J Med. 1995;332:201–8. - PubMed
-
- Mellors JW, Rinaldo CR, Gupta P, et al. Prognosis in HIV-1 infection predicted by the quantity of virus in the plasma. Science. 1996;272:1167–70. - PubMed
-
- O'Brien WA, Hartigan PM, Martin D, et al. Changes in plasma HIV-1 RNA and CD4+ lymphocyte count and the risk of progression to AIDS. N Engl J Med. 1996;334:426–31. - PubMed
-
- Katzenstein DA, Hammer SM, Hugues MD, et al. The relation of virologic and immunologic marker to clinical outcomes after nucleoside therapy in HIV-infected adults. N Engl J Med. 1996;335:1091–8. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
