

Long-term outcomes of regional variations in intensity of invasive vs medical management of Medicare Patients with acute myocardial infarction
- PMID: 15769966
- PMCID: PMC1459288
- DOI: 10.1001/jama.293.11.1329
Long-term outcomes of regional variations in intensity of invasive vs medical management of Medicare Patients with acute myocardial infarction
Abstract
Context: The health and policy implications of the marked regional variations in intensity of invasive compared with medical management of patients with acute myocardial infarction (AMI) are unknown.
Objectives: To evaluate patient clinical characteristics associated with receiving more intensive treatment; and to assess whether AMI patients residing in regions with more intensive invasive treatment and management strategies have better long-term survival than those residing in regions with more intensive medical management strategies.
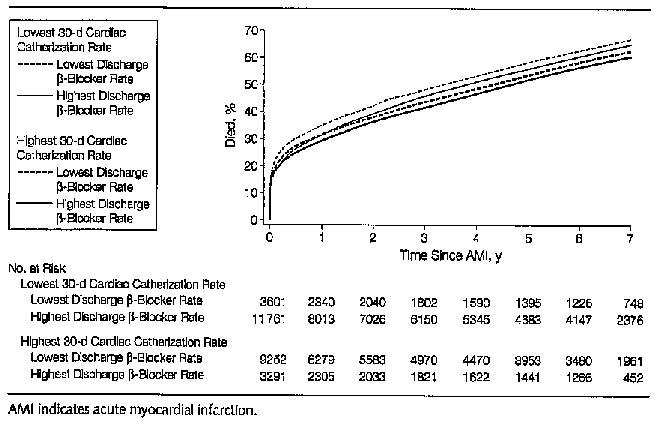
Design, setting, and patients: National cohort study of 158,831 elderly Medicare patients hospitalized with first episode of confirmed AMI in 1994-1995, followed up for 7 years (mean, 3.6 years), according to the intensity of invasive management (performance of cardiac catheterization within 30 days) and medical management (prescription of beta-blockers to appropriate patients at discharge) in their region of residence. Baseline chart reviews were drawn from the Cooperative Cardiovascular Project and linked to Medicare health administrative data.
Main outcome measure: Long-term survival over 7 years of follow-up.
Results: Patient baseline AMI severity was similar across regions. In all regions, younger and healthier patients were more likely than older high-risk patients to receive invasive treatment and medical therapy. Regions with more invasive treatment practice styles had more cardiac catheterization laboratory capacity; patients in these regions were more likely to receive interventional treatment, regardless of age, clinical indication, or risk profile. The absolute unadjusted difference in 7-year survival between regions providing the highest rates of both invasive and medical management strategies and those providing the lowest rates of both was 6.2%. For both ST- and non-ST-segment elevation AMI patients, survival improved with regional intensity of both invasive and medical management. In areas with higher rates of medical management, there appeared to be little or no improvement in survival associated with increased invasive treatment.
Conclusions: In elderly Medicare patients with AMI, more intensive medical treatment provides population survival benefits. However, routine use of more costly and invasive treatment strategies may not be associated with an overall population benefit beyond that seen with excellent medical management. Efforts should focus on directing invasive clinical resources to patients with the greatest expected benefit.
Figures
Similar articles
-
Regional variation in cardiac catheterization appropriateness and baseline risk after acute myocardial infarction.J Am Coll Cardiol. 2008 Feb 19;51(7):716-23. doi: 10.1016/j.jacc.2007.10.039. J Am Coll Cardiol. 2008. PMID: 18279735
-
Association between hospital cardiac management and outcomes for acute myocardial infarction patients.Med Care. 2010 Feb;48(2):157-65. doi: 10.1097/MLR.0b013e3181bd4da7. Med Care. 2010. PMID: 19927014
-
National use and effectiveness of beta-blockers for the treatment of elderly patients after acute myocardial infarction: National Cooperative Cardiovascular Project.JAMA. 1998 Aug 19;280(7):623-9. doi: 10.1001/jama.280.7.623. JAMA. 1998. PMID: 9718054
-
Acute coronary care in the elderly, part I: Non-ST-segment-elevation acute coronary syndromes: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology.Circulation. 2007 May 15;115(19):2549-69. doi: 10.1161/CIRCULATIONAHA.107.182615. Circulation. 2007. PMID: 17502590 Review.
-
API expert consensus document on management of ischemic heart disease.J Assoc Physicians India. 2006 Jun;54:469-80. J Assoc Physicians India. 2006. PMID: 16909697 Review.
Cited by
-
Association Between Claims-Defined Frailty and Outcomes Following 30 Versus 12 Months of Dual Antiplatelet Therapy After Percutaneous Coronary Intervention: Findings From the EXTEND-DAPT Study.J Am Heart Assoc. 2023 Jul 18;12(14):e029588. doi: 10.1161/JAHA.123.029588. Epub 2023 Jul 14. J Am Heart Assoc. 2023. PMID: 37449567 Free PMC article. Clinical Trial.
-
Temporal trends in the utilization of diagnostic testing and treatments for cardiovascular disease in the United States, 1993-2001.Circulation. 2006 Jan 24;113(3):374-9. doi: 10.1161/CIRCULATIONAHA.105.560433. Circulation. 2006. PMID: 16432068 Free PMC article.
-
ESTIMATING MARGINAL RETURNS TO MEDICAL CARE: EVIDENCE FROM AT-RISK NEWBORNS.Q J Econ. 2010 May 1;125(2):591-634. doi: 10.1162/qjec.2010.125.2.591. Q J Econ. 2010. PMID: 20634927 Free PMC article.
-
Determinants of cardiac catheterization use in older Medicare patients with acute myocardial infarction.Circ Cardiovasc Qual Outcomes. 2010 Jan;3(1):54-62. doi: 10.1161/CIRCOUTCOMES.109.858456. Epub 2009 Dec 8. Circ Cardiovasc Qual Outcomes. 2010. PMID: 20123672 Free PMC article.
-
Positive troponin in diabetic ketoacidosis without evident acute coronary syndrome predicts adverse cardiac events.Clin Cardiol. 2008 Feb;31(2):67-71. doi: 10.1002/clc.20167. Clin Cardiol. 2008. PMID: 18257021 Free PMC article.
References
-
- Wennberg DE; Dartmouth Atlas of Cardiovascular Health Care Working Group. The Dartmouth Atlas of Cardiovascular Health Care Chicago, III: AHA Press; 1999.
-
- Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. - PubMed
-
- Boden WE, O’Rourke RA, Crawford MH, et al. Veterans Affairs Non-Q-Wave infarction Strategies in Hospital (VANQWISH) Trial investigators. Outcomes in patients with acute non-Q-wave myocardial infarction randomly assigned to an invasive as compared with a conservative management strategy. N Engl J Med. 1998;338:1785–1792. - PubMed
-
- Cannon CP, Weintraub WS, Demopoulos LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879–1887. - PubMed
-
- Fox KA, Poole-Wilson PA, Henderson RA, et al. Interventional versus conservative treatment for patients with unstable angina or non-ST-elevation myocardial infarction: the British Heart Foundation RITA 3 randomised trial: Randomized intervention Trial of unstable Angina. Lancet. 2002;360:743–751. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
