

Evaluation of the pattern of treatment, level of anticoagulation control, and outcome of treatment with warfarin in patients with non-valvar atrial fibrillation: a record linkage study in a large British population
- PMID: 15772203
- PMCID: PMC1768813
- DOI: 10.1136/hrt.2004.042465
Evaluation of the pattern of treatment, level of anticoagulation control, and outcome of treatment with warfarin in patients with non-valvar atrial fibrillation: a record linkage study in a large British population
Abstract
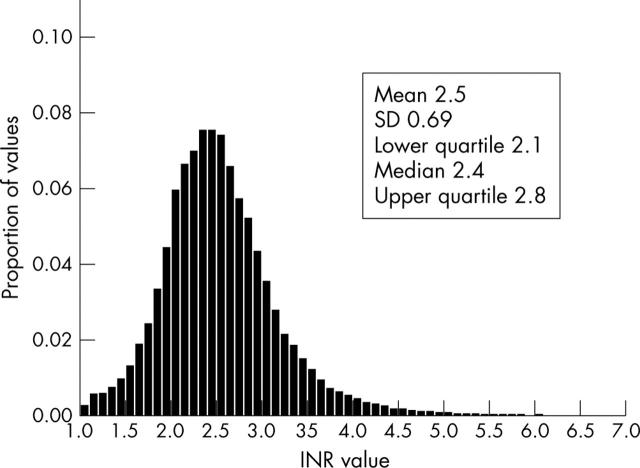
Objective: To evaluate how well patients with non-valvar atrial fibrillation (NVAF) were maintained within the recommended international normalised ratio (INR) target of 2.0-3.0 and to explore the relation between achieved INR control and clinical outcomes.
Design: Record linkage study of routine activity records and INR measurements.
Setting: Cardiff and the Vale of Glamorgan, South Wales, UK.
Participants: 2223 patients with NVAF, no history of heart valve replacement, and with at least five INR measurements.
Main outcome measures: Mortality, ischaemic stroke, all thromboembolic events, bleeding events, hospitalisation, and patterns of INR monitoring.
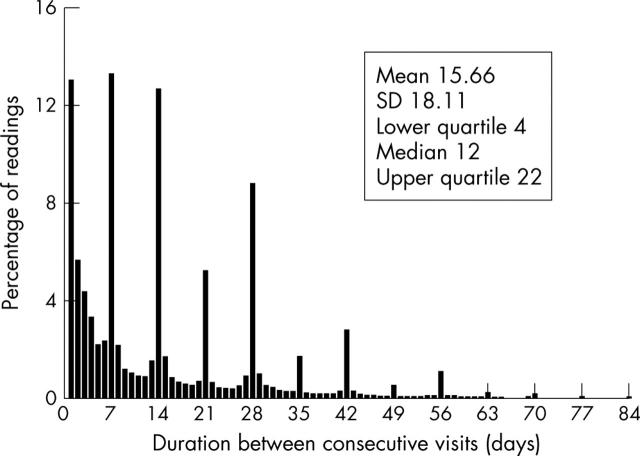
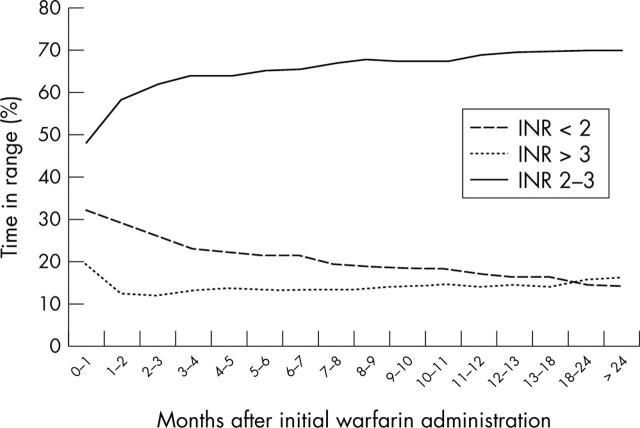
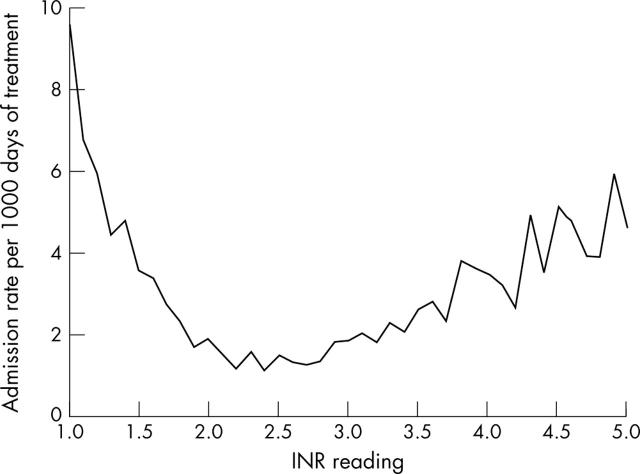
Results: Patients treated with warfarin were outside the INR target range 32.1% of the time, with 15.4% INR values > 3.0 and 16.7% INR values < 2.0. However, the quartile with worst control spent 71.6% of their time out of target range compared with only 16.3% out of range in the best controlled quartile. The median period between INR tests was 16 days. Time spent outside the target range decreased as the duration of INR monitoring increased, from 52% in the first three months of monitoring to 30% after two years. A multivariate logistic regression model showed that a 10% increase in time out of range was associated with an increased risk of mortality (odds ratio (OR) 1.29, p < 0.001) and of an ischaemic stroke (OR 1.10, p = 0.006) and other thromboembolic events (OR 1.12, p < 0.001). The rate of hospitalisation was higher when INR was outside the target range.
Conclusions: Suboptimal anticoagulation was associated with poor clinical outcomes, even in a well controlled population. However, good control was difficult to achieve and maintain. New measures are needed to improve maintenance anticoagulation in patients with NVAF.
Figures
Comment in
-
Atrial fibrillation: will new drugs and patient choice improve anticoagulation outcomes?Heart. 2005 Apr;91(4):423-4. doi: 10.1136/hrt.2004.047902. Heart. 2005. PMID: 15772185 Free PMC article.
-
How good is anticoagulation control in non-valvar atrial fibrillation? Observations on the elderly, ethnicity, patient perceptions, and understanding of AF thromboprophylaxis.Heart. 2005 Apr;91(4):425-6. doi: 10.1136/hrt.2004.052480. Heart. 2005. PMID: 15772186 Free PMC article.
Similar articles
-
Evaluation of survival and ischaemic and thromboembolic event rates in patients with non-valvar atrial fibrillation in the general population when treated and untreated with warfarin.Heart. 2006 Feb;92(2):196-200. doi: 10.1136/hrt.2004.058339. Epub 2005 May 9. Heart. 2006. PMID: 15883133 Free PMC article.
-
Anticoagulation in patients with non-valvular atrial fibrillation: an evaluation of stability and early factors that predict longer-term stability on warfarin in a large UK population.Curr Med Res Opin. 2005 Dec;21(12):1905-13. doi: 10.1185/030079905X75050. Curr Med Res Opin. 2005. PMID: 16368039
-
Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation.N Engl J Med. 2003 Sep 11;349(11):1019-26. doi: 10.1056/NEJMoa022913. N Engl J Med. 2003. PMID: 12968085
-
Is it safe to stop anticoagulants after successful surgery for atrial fibrillation?Interact Cardiovasc Thorac Surg. 2011 Dec;13(6):642-8. doi: 10.1510/icvts.2011.282319. Epub 2011 Sep 1. Interact Cardiovasc Thorac Surg. 2011. PMID: 21885540 Review.
-
Optimal INR for prevention of stroke and death in atrial fibrillation: a critical appraisal.Thromb Res. 2006;117(5):493-9. doi: 10.1016/j.thromres.2004.11.025. Epub 2004 Dec 25. Thromb Res. 2006. PMID: 16517250 Review.
Cited by
-
Dabigatran for the prevention of stroke and systemic embolism in atrial fibrillation: A NICE single technology appraisal.Pharmacoeconomics. 2013 Jul;31(7):551-62. doi: 10.1007/s40273-013-0051-8. Pharmacoeconomics. 2013. PMID: 23620211 Review.
-
Practical use of dabigatran etexilate for stroke prevention in atrial fibrillation.Int J Clin Pract. 2013 Jun;67(6):516-26. doi: 10.1111/ijcp.12147. Epub 2013 Apr 5. Int J Clin Pract. 2013. PMID: 23557519 Free PMC article. Review.
-
Bleeding events and associated factors in a cohort of adult patients taking warfarin in Sarawak, Malaysia.J Thromb Thrombolysis. 2014;38(2):226-34. doi: 10.1007/s11239-013-1017-6. J Thromb Thrombolysis. 2014. PMID: 24233388
-
[Pharmacogenetics. Clinical relevance in anesthsiology].Anaesthesist. 2013 Nov;62(11):874-86. doi: 10.1007/s00101-013-2233-3. Anaesthesist. 2013. PMID: 24275933 Review. German.
-
Genetic and Non-Genetic Factors Impact on INR Normalization in Preprocedural Warfarin Management.Pharmgenomics Pers Med. 2021 Aug 28;14:1069-1080. doi: 10.2147/PGPM.S322743. eCollection 2021. Pharmgenomics Pers Med. 2021. PMID: 34483679 Free PMC article.
References
-
- Chatap G, Giraud K, Vincent JP. Atrial fibrillation in the elderly: facts and management. Drugs Aging 2002;19:819–46. - PubMed
-
- Department of Health. National framework for older people. Standard 5: stroke. London: Stationery Office, 2001.
-
- EAFT Study Group. Secondary prevention in non-rheumatic atrial fibrillation after transient ischaemic attack or minor stroke. EAFT (European atrial fibrillation trial) Study Group. Lancet 1993;342:1255–62. - PubMed
-
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation: analysis of pooled data from five randomised controlled trials. Arch Intern Med 1994;154:1449–57. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical