

Incomplete functional recovery after delirium in elderly people: a prospective cohort study
- PMID: 15774005
- PMCID: PMC1079829
- DOI: 10.1186/1471-2318-5-5
Incomplete functional recovery after delirium in elderly people: a prospective cohort study
Abstract
Background: Delirium often has a poor outcome, but why some people have incomplete recovery is not well understood. Our objective was to identify factors associated with short-term (by discharge) and long-term (by 6 month) incomplete recovery of function following delirium.
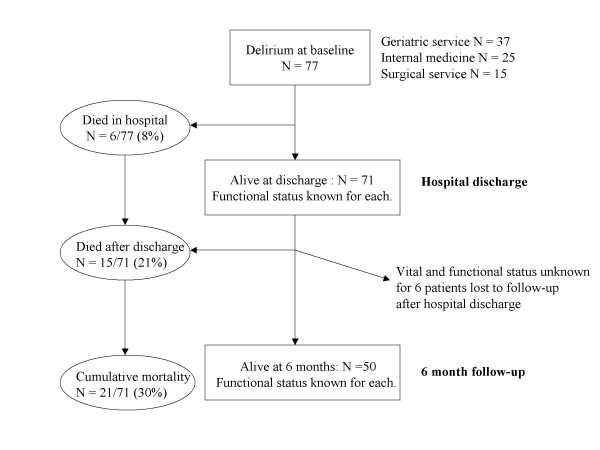
Methods: In a prospective cohort study of elderly patients with delirium seen by geriatric medicine services, function was assessed at baseline, at hospital discharge and at six months.
Results: Of 77 patients, vital and functional status at 6 months was known for 71, of whom 21 (30%) had died. Incomplete functional recovery, defined as > or =10 point decline in the Barthel Index, compared to pre-morbid status, was present in 27 (54%) of the 50 survivors. Factors associated with death or loss of function at hospital discharge were frailty, absence of agitation (hypoactive delirium), a cardiac cause and poor recognition of delirium by the treating service. Frailty, causes other than medications, and poor recognition of delirium by the treating service were associated with death or poor functional recovery at 6 months.
Conclusion: Pre-existing frailty, cardiac cause of delirium, and poor early recognition by treating physicians are associated with worse outcomes. Many physicians view the adverse outcomes of delirium as intractable. While in some measure this might be true, more skilled care is a potential remedy within their grasp.
Similar articles
-
Recovery of functional impairment after acute illness and mortality: one-year follow-up study.Gerontology. 2009;55(3):269-74. doi: 10.1159/000193068. Epub 2009 Jan 12. Gerontology. 2009. PMID: 19141990
-
Impact of frailty and residual subsyndromal delirium on 1-year functional recovery: A prospective cohort study.Geriatr Gerontol Int. 2017 Dec;17(12):2472-2478. doi: 10.1111/ggi.13108. Epub 2017 Jun 22. Geriatr Gerontol Int. 2017. PMID: 28639340
-
Illness presentation in elderly patients.Arch Intern Med. 1995 May 22;155(10):1060-4. Arch Intern Med. 1995. PMID: 7748049
-
Delirium in the elderly patient.Am Fam Physician. 1994 Nov 1;50(6):1325-32. Am Fam Physician. 1994. PMID: 7942430 Review.
-
Predisposing and precipitating factors for delirium in a frail geriatric population.J Psychosom Res. 2008 Sep;65(3):249-54. doi: 10.1016/j.jpsychores.2008.05.026. J Psychosom Res. 2008. PMID: 18707947 Review.
Cited by
-
Using consensus methods to prioritize modifiable risk factors for development of manifestations of frailty in hospitalized older adults.Nurs Open. 2023 Feb;10(2):1016-1028. doi: 10.1002/nop2.1370. Epub 2022 Sep 26. Nurs Open. 2023. PMID: 36161707 Free PMC article.
-
Prevalence of delirium in German nursing homes: protocol for a cross-sectional study.BMJ Open. 2025 Jan 15;15(1):e087482. doi: 10.1136/bmjopen-2024-087482. BMJ Open. 2025. PMID: 39819912 Free PMC article.
-
Delirium prevalence and delirium literacy across Italian hospital wards: a secondary analysis of data from the World Delirium Awareness Day 2023.Eur Geriatr Med. 2024 Oct;15(5):1405-1413. doi: 10.1007/s41999-024-01019-5. Epub 2024 Jul 18. Eur Geriatr Med. 2024. PMID: 39023695 Free PMC article.
-
Impact of Hospitalization on Patients Ability to Perform Basic Activities of Daily Living.Can Geriatr J. 2023 Dec 1;26(4):524-529. doi: 10.5770/cgj.26.664. eCollection 2023 Dec. Can Geriatr J. 2023. PMID: 38045878 Free PMC article.
-
A Scoping Review of Frailty and Acute Care in Middle-Aged and Older Individuals with Recommendations for Future Research.Can Geriatr J. 2017 Mar 31;20(1):22-37. doi: 10.5770/cgj.20.240. eCollection 2017 Mar. Can Geriatr J. 2017. PMID: 28396706 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
