

Retinal dysfunction and refractive errors: an electrophysiological study of children
- PMID: 15774929
- PMCID: PMC1772604
- DOI: 10.1136/bjo.2004.045328
Retinal dysfunction and refractive errors: an electrophysiological study of children
Abstract
Aims: To evaluate the relation between refractive error and electrophysiological retinal abnormalities in children referred for investigation of reduced vision.
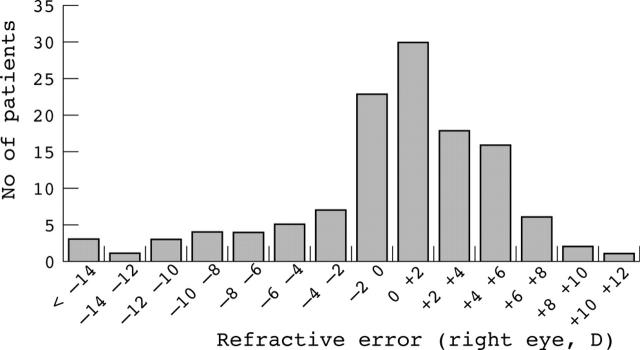
Methods: The study group comprised 123 consecutive patients referred over a 14 month period from the paediatric service of Moorfields Eye Hospital for electrophysiological investigation of reduced vision. Subjects were divided into five refractive categories according to their spectacle correction: high myopia (< or = -6D), low myopia (>-6D and < or = -0.75D), emmetropia (>-0.75 and <1.5D), low hyperopia (> or = 1.5 and <6D), and high hyperopia (> or = 6D). Patients with a specific diagnosis at the time of electrophysiological testing were excluded. Only the first member of any one family was included if more than one sibling had been tested. All tests were performed to incorporate ISCEV standards, using gold foil corneal electrodes where possible. In younger patients skin electrodes and an abbreviated protocol were employed.
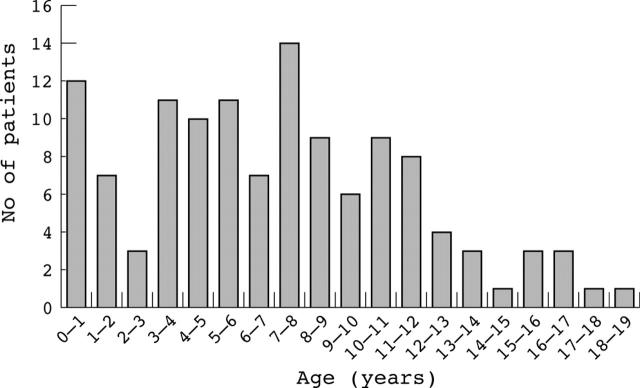
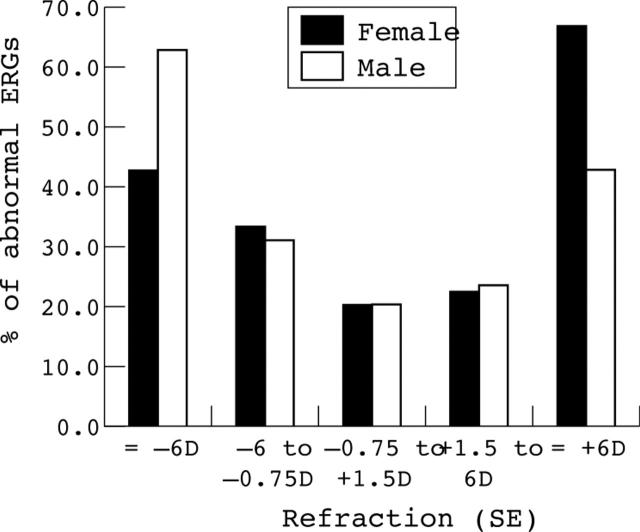
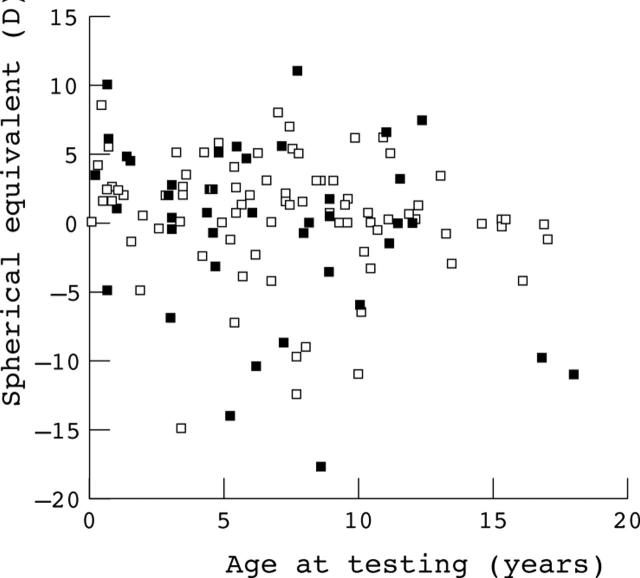
Results: The mean age of patients was 7.1 years with an overall incidence of abnormal electrophysiological findings of 29.3%. The incidence of abnormality was higher in high ametropes (13/25, 52%) compared to the other groups (23/98, 23.5%). This difference was statistically significant (chi2 test, p = 0.005). There was also a significant association between high astigmatism (>1.5D) and ERG abnormalities (18/35 with high astigmatism v 20/88 without, chi2 test, p = 0.002). There was no significant variation in frequency of abnormalities between low myopes, emmetropes, and low hyperopes. The rate of abnormalities was very similar in both high myopes (8/15) and high hyperopes (5/10).
Conclusions: High ametropia and astigmatism in children being investigated for poor vision are associated with a higher rate of retinal electrophysiological abnormalities. An increased rate of refractive errors in the presence of retinal pathology is consistent with the hypothesis that the retina is involved in the process of emmetropisation. Electrophysiological testing should be considered in cases of high ametropia in childhood to rule out associated retinal pathology.
Figures
References
-
- Laties AM, Stone RA. Ametropia in retinal disorders. Ch 35. In: Anderson RE, Hollyfield JG, LaVail MM, eds. Retinal degenerations Boca Raton, CRC Press 1991:383–90.
-
- Fulton AB, Hansen RM, Mayer DL. Vision in Leber congenital amaurosis. Arch Ophthalmol 1996;114:698–703. - PubMed
-
- Hirashima S, Ohba N. A pedigree of Leber’s congenital amaurosis. Ophthalmic Paediatr Genet 1988;9:29–36. - PubMed
-
- Zito I, Allen LE, Patel RJ, et al. Mutations in the CACNA1F and NYX genes in British CSNBX families. Hum Mutat 2003;21:169. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical