

Outcome of endovascular treatment in symptomatic intracranial vascular stenosis
- PMID: 15782013
- PMCID: PMC2684991
- DOI: 10.3348/kjr.2005.6.1.1
Outcome of endovascular treatment in symptomatic intracranial vascular stenosis
Abstract
Objective: The outcome evaluation for the revascularization of intracranial vascular stenoses has not been fully described due to the highly technical nature of the procedure. We report here on the early and late clinical outcomes of angioplasty and/or stenting of symptomatic severe intracranial vascular stenoses at a single institute.
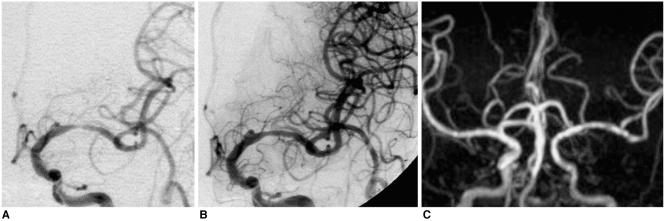
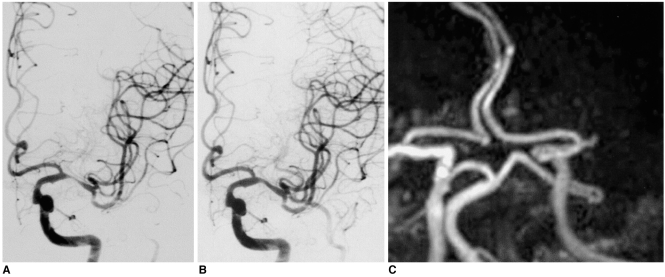
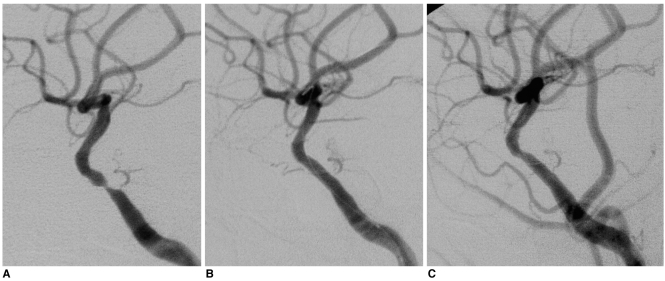
Materials and methods: Since 1995, we have treated 35 patients with symptomatic intracranial vascular stenosis (more than 70% stenosis, mean stenosis: 78.6%+/-6.2%). Angioplasty (n = 19) was performed for the horizontal segment of the middle cerebral artery (M1) (n = 16) and the basilar artery (BA) (n = 1), the intradural vertebral artery (VA) (n = 1), and the cavernous internal carotid artery (ICA) (n = 1). Stenting (n = 16) was performed for the cavernous or petrous ICAs (n = 9), the intradural VA (n = 3), BA (n = 2), and M1 (n = 2) artery. We assessed the angiographic success (defined as residual stenosis < 50%) rate, the periprocedural complications during the 30-day periprocedural period, the symptomatic recurrence and restenosis during a mean 22-month follow-up (FU) period. The Kaplan-Meier estimate of the cumulative event-free rate of the major cerebrovascular events, i.e. death, stroke or restenosis, was also done.
Results: Angiographic success was achieved in 97% of our patients (34/35). There were four procedure-related complications (11%) including a death and a minor stroke. During the mean 22-month FU, the asymptomatic restenosis rate was 9% and the symptomatic restenosis rate was 6% in the target lesion and 9% in all the vascular territories. The Kaplan-Meier estimate was 70.6% (95% confidence interval = 46.5-94.7) after 33 months of FU.
Conclusion: In addition to a high angiographic success rate and an acceptable periprocedural complication rate, intracranial angioplasty and/or stenting revealed a relatively low symptomatic recurrence rate. Hemorrhage is a rare, but the physician must aware that potentially fatal periprocedural complications can occur.
Figures
References
-
- Sacco RL, Kargman DE, Gu Q, Zamanillo MC. Race-ethnicity and determinants of intracranial atherosclerotic cerebral infarction. The Northern Manhattan Stroke Study. Stroke. 1995;26:14–20. - PubMed
-
- Wityk RJ, Lehman D, Klag M, Coresh J, Ahn H, Litt B. Race and sex differences in the distribution of cerebral atherosclerosis. Stroke. 1996;27:1974–1980. - PubMed
-
- Lee SJ, Cho SJ, Moon HS, Shon YM, Lee KH, Kim DI, et al. Combined extracranial and intracranial atherosclerosis in Korean patients. Arch Neurol. 2003;60:1561–1564. - PubMed
-
- Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) Trial Investigators. Design, progress and challenges of a double-blind trial of warfarin versus aspirin for symptomatic intracranial arterial stenosis. Neuroepidemiology. 2003;22:106–117. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
