

Immunohistochemical, in situ hybridization, and ultrastructural localization of SARS-associated coronavirus in lung of a fatal case of severe acute respiratory syndrome in Taiwan
- PMID: 15791576
- PMCID: PMC7112064
- DOI: 10.1016/j.humpath.2004.11.006
Immunohistochemical, in situ hybridization, and ultrastructural localization of SARS-associated coronavirus in lung of a fatal case of severe acute respiratory syndrome in Taiwan
Abstract
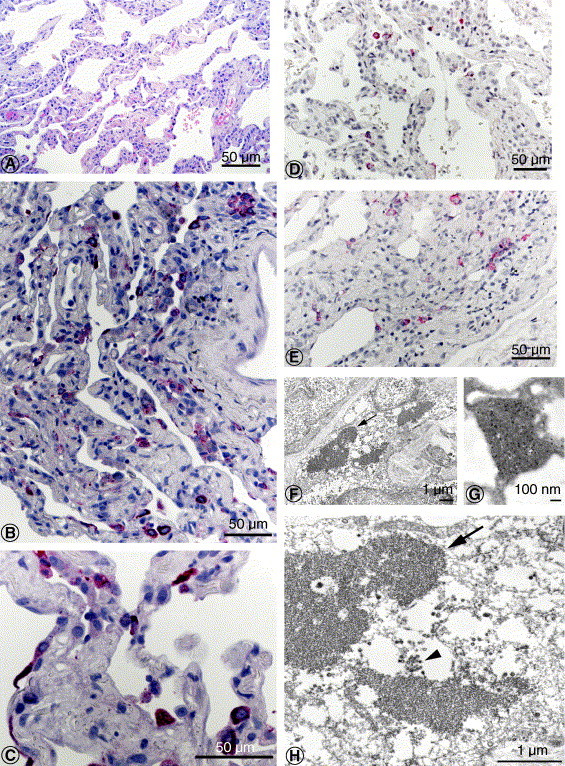
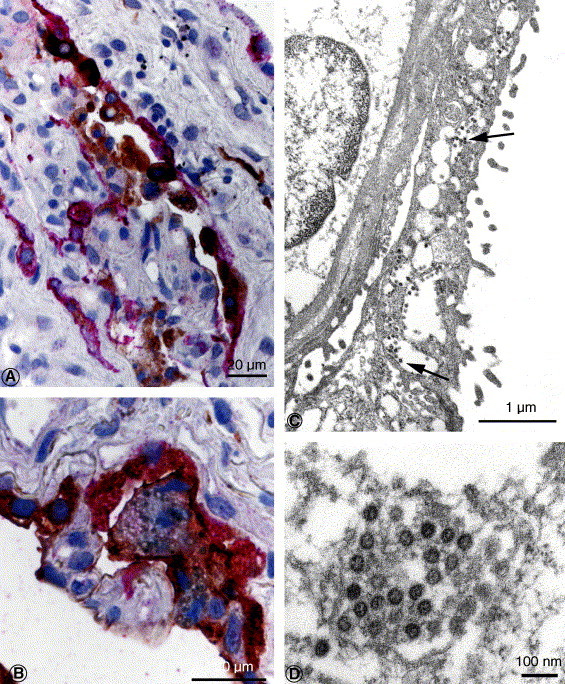
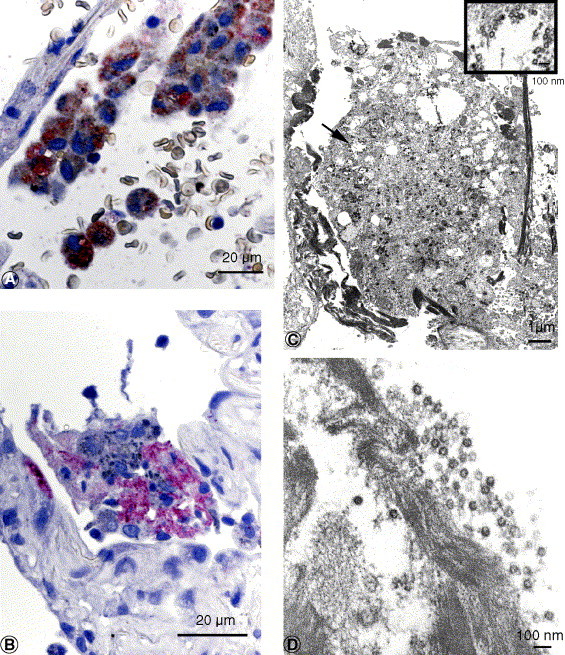
This article describes the pathological studies of fatal severe acute respiratory syndrome (SARS) in a 73-year-old man during an outbreak of SARS in Taiwan, 2003. Eight days before onset of symptoms, he visited a municipal hospital that was later identified as the epicenter of a large outbreak of SARS. On admission to National Taiwan University Hospital in Taipei, the patient experienced chest tightness, progressive dyspnea, and low-grade fever. His condition rapidly deteriorated with increasing respiratory difficulty, and he died 7 days after admission. The most prominent histopathologic finding was diffuse alveolar damage of the lung. Immunohistochemical and in situ hybridization assays demonstrated evidence of SARS-associated coronavirus (SARS-CoV) infection in various respiratory epithelial cells, predominantly type II pneumocytes, and in alveolar macrophages in the lung. Electron microscopic examination also revealed coronavirus particles in the pneumocytes, and their identity was confirmed as SARS-CoV by immunogold labeling electron microscopy. This report is the first to describe the cellular localization of SARS-CoV in human lung tissue by using a combination of immunohistochemistry, double-stain immunohistochemistry, in situ hybridization, electron microscopy, and immunogold labeling electron microscopy. These techniques represent valuable laboratory diagnostic modalities and provide insights into the pathogenesis of this emerging infection.
Figures
References
-
- WHO issues consensus document on the epidemiology of SARS. Wkly. Epidemiol. Rec. 2003;78:373–375. - PubMed
-
- Ksiazek T.G., Erdman D., Goldsmith C.S. A novel coronavirus associated with severe acute respiratory syndrome. N. Engl. J. Med. 2003;348(20):1953–1966. - PubMed
-
- Nakajima N., Asahi-Ozaki Y., Nagata N. SARS coronavirus-infected cells in lung detected by new in situ hybridization technique. Jpn. J. Infect. Dis. 2003;56(3):139–141. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
