

Protection from cytomegalovirus after transplantation is correlated with immediate early 1-specific CD8 T cells
- PMID: 15795239
- PMCID: PMC2213133
- DOI: 10.1084/jem.20042384
Protection from cytomegalovirus after transplantation is correlated with immediate early 1-specific CD8 T cells
Abstract
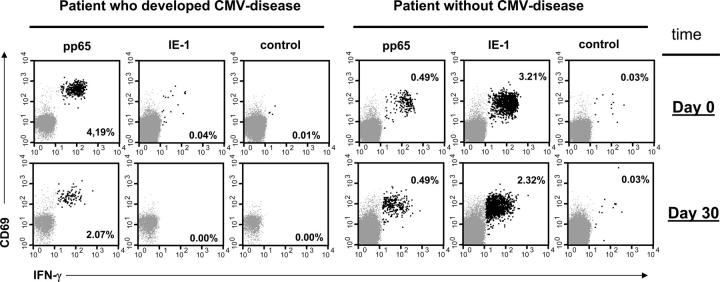
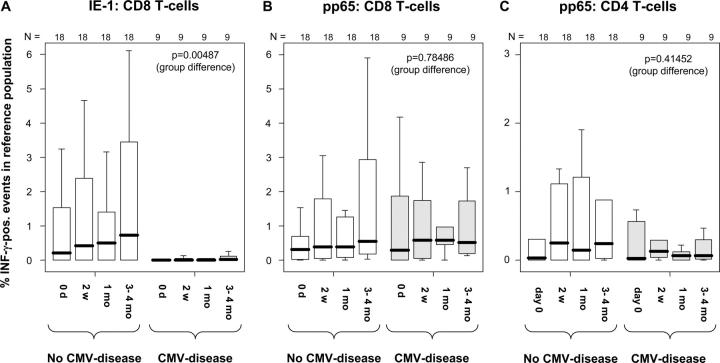
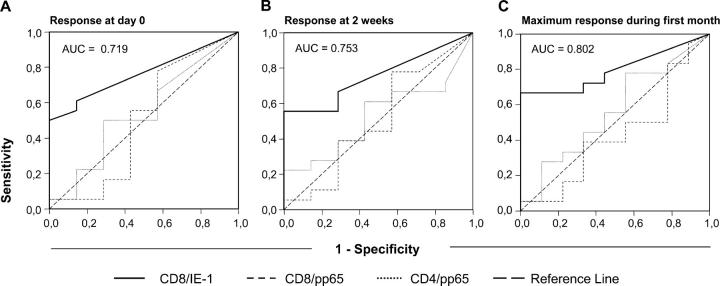
T cells are crucial for the control of cytomegalovirus (CMV) in infected individuals. Although CMV-specific T cells can be quantified by various methods, clear correlates of protection from CMV disease have not been defined. However, responses to the pp65 protein are believed to play an important role. Here, the proportions of interferon gamma-producing T cells following ex vivo activation with pools of overlapping peptides representing the pp65 and immediate early (IE)-1 proteins were determined at multiple time points and related to the development of CMV disease in 27 heart and lung transplant recipients. Frequencies of IE-1-specific CD8 T cells above 0.2 and 0.4% at day 0 and 2 wk, respectively, or 0.4% at any time during the first months discriminated patients who did not develop CMV disease from patients at risk, 50-60% of whom developed CMV disease. No similar distinction between risk groups was possible based on pp65-specific CD8 or CD4 T cell responses. Remarkably, CMV disease developed exclusively in patients with a dominant pp65-specific CD8 T cell response. In conclusion, high frequencies of IE-1 but not pp65-specific CD8 T cells correlate with protection from CMV disease. These results have important implications for monitoring T cell responses, adoptive cell therapy, and vaccine design.
Figures
References
-
- Toro, A.I., and J. Ossa. 1996. PCR activity of CMV in healthy CMV-seropositive individuals: does latency need redefinition? Res. Virol. 147:233–238. - PubMed
-
- Fishman, J.A., and R.H. Rubin. 1998. Infection in organ-transplant recipients. N. Engl. J. Med. 338:1741–1751. - PubMed
-
- Quinnan, G.V., Jr., N. Kirmani, A.H. Rook, J.F. Manischewitz, L. Jackson, G. Moreschi, G.W. Santos, R. Saral, and W.H. Burns. 1982. Cytotoxic T cells in cytomegalovirus infection: HLA-restricted T-lymphocyte and non-T-lymphocyte cytotoxic responses correlate with recovery from cytomegalovirus infection in bone-marrow-transplant recipients. N. Engl. J. Med. 307:7–13. - PubMed
-
- Guiver, M., A.J. Fox, K. Mutton, N. Mogulkoc, and J. Egan. 2001. Evaluation of CMV viral load using TaqMan CMV quantitative PCR and comparison with CMV antigenemia in heart and lung transplant recipients. Transplantation. 71:1609–1615. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
