

Effects of making emergency contraception available without a physician's prescription: a population-based study
- PMID: 15795408
- PMCID: PMC554872
- DOI: 10.1503/cmaj.045019
Effects of making emergency contraception available without a physician's prescription: a population-based study
Erratum in
- CMAJ. 2005 Apr 26;172(9):1164
Abstract
Background: Timely access to emergency contraception has the potential to reduce the number of unwanted pregnancies and subsequent abortions. A public health policy initiative in British Columbia beginning in December 2000 allowed pharmacists to provide emergency contraceptives (ECs) without a prescription. We sought to determine changes in EC use after the policy was introduced and to analyze EC use with data generated by the policy.
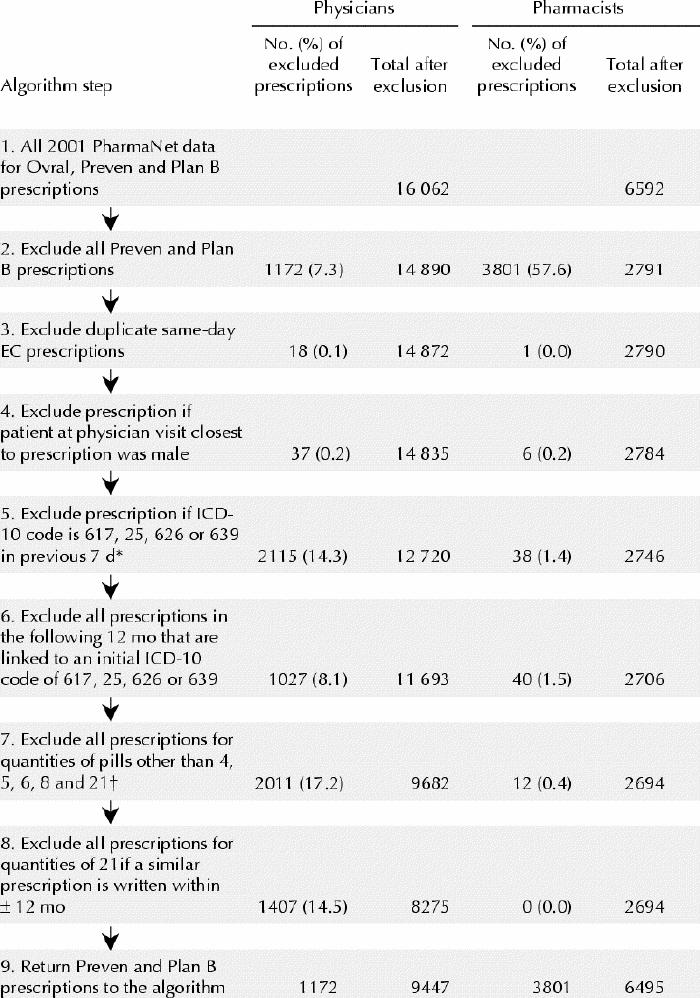
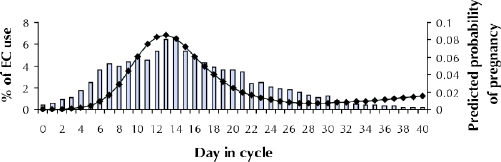
Methods: All Ovral, Preven and Plan B EC prescriptions from Jan. 1, 1996, to Dec. 31, 2003, were identified through the BC PharmaNet and Medical Services Plan administrative databases and the data analyzed to determine changes between 1996 and 2002. Changes over time were determined in the frequency of EC provision, choice of EC agent, frequency of EC use by age group, repeat use and geographic distribution of EC prescription for the pre- and post-policy periods. Anonymized patient-specific data from treatment consent forms were used to describe the reason for EC use, interval between unprotected intercourse and EC prescription, proportion prescribed for immediate or future use, referrals for regular birth control and STD screening and concomitant antiemetic use. Consent data also provided the time in the menstrual cycle that the EC was requested.
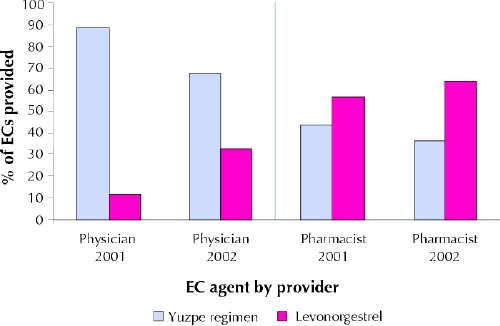
Results: The number of EC prescriptions increased from a pre-policy mean of 8805 (99% confidence interval 7823-9787) in the years 1996 to 2000 to a post-policy total in 2002 of 17 794. Physicians prescribed the levonorgestrel regimen (Plan B) less frequently than did pharmacists. The frequency of EC use was highest among women aged 20-24 years across all study years, and all age groups demonstrated a post-policy increase in use. On average, 2.1% of the women received an EC 3 or more times a year over the period of the study. More women in urban regions received ECs than women in more rural areas of the province. Analysis of pharmacist treatment consent forms used in 2001 and 2002 showed that 56.2% of women receiving an EC reported using a method of birth control that had failed, 55.7% of pharmacist-provided ECs were obtained within 24 hours after unprotected intercourse, 1.1% of ECs were obtained for future use, antiemetics were provided to 57.7% of women receiving the Yuzpe regimen (Ovral, Preven) and to 20.5% of women receiving levonorgestrel, and women tended to seek ECs when unprotected intercourse occurred at the time of highest risk of pregnancy in their menstrual cycle. Women in greatest financial need obtained ECs more frequently from physicians than from pharmacists.
Interpretation: The policy change that granted pharmacists authority to provide ECs to women without a physician's prescription did not simply expand EC availability but was associated with an overall increase in EC use in the province.
Figures
References
-
- Jones RK, Darroch JE, Henshaw SK. Contraceptive use among US women having abortions in 2000–2001. Perspect Sex Reprod Health 2002;34:294-303. - PubMed
-
- BC Vital Statistics Agency. Pregnancy rates by health authority: British Columbia, 1993 to 2001. Victoria, BC: British Columbia Vital Statistics Agency; 2003.
-
- Task Force on Postovulatory Methods of Fertility Regulation. Randomised controlled trial of levonorgestrel versus the Yuzpe regimen of combined oral contraceptives for emergency contraception. Lancet 1998;352:428-33. - PubMed
-
- Piaggio G, von Hertzen H, Grimes DA, Van Look PFA. Timing of emergency contraception with levonorgestrel or the Yuzpe regimen. Task Force on Postovulatory Methods of Fertility Regulation. Lancet 1998;353:721. - PubMed
-
- Norris Turner A, Ellertson C. How safe is emergency contraception? Drug Safety 2002;25:695-706. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials