

Current perceptions regarding surgical margin status after breast-conserving therapy: results of a survey
- PMID: 15798465
- PMCID: PMC1357067
- DOI: 10.1097/01.sla.0000157272.04803.1b
Current perceptions regarding surgical margin status after breast-conserving therapy: results of a survey
Abstract
Objective: The surgical margin status after breast-conserving surgery is considered the strongest predictor for local failure. The purpose of this study is to survey how radiation oncologists in North America (NA) and Europe define negative or close surgical margins after lumpectomy and to determine the factors that govern the decision to recommend reexcision based on the margins status.
Methods: A questionnaire was sent to active members of the European Society of Therapeutic Radiation Oncology and the American Society for Therapeutic Radiology and Oncology who had completed training in radiation oncology. Respondents were asked whether they would characterize margins to be negative or close for a variety of scenarios. A second survey was sent to 500 randomly selected radiation oncologists in the United States to assess when a reexcision would be recommended based on surgical margins.
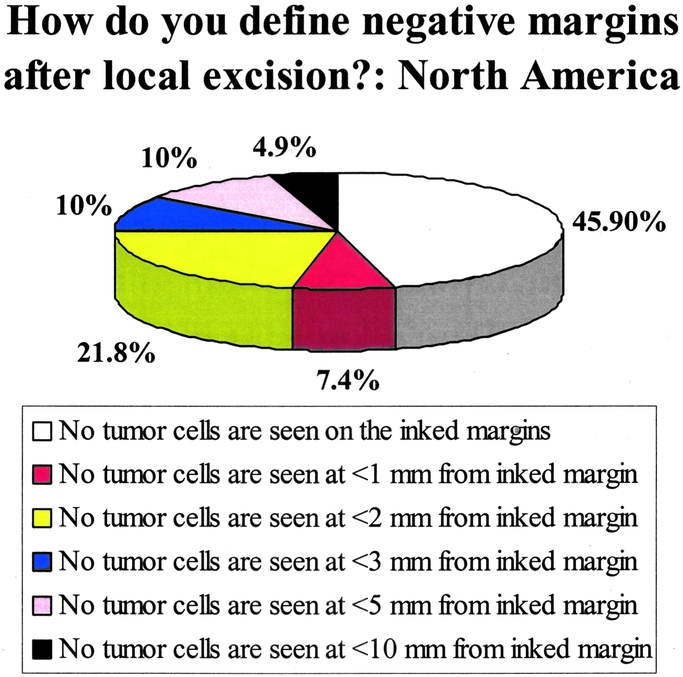
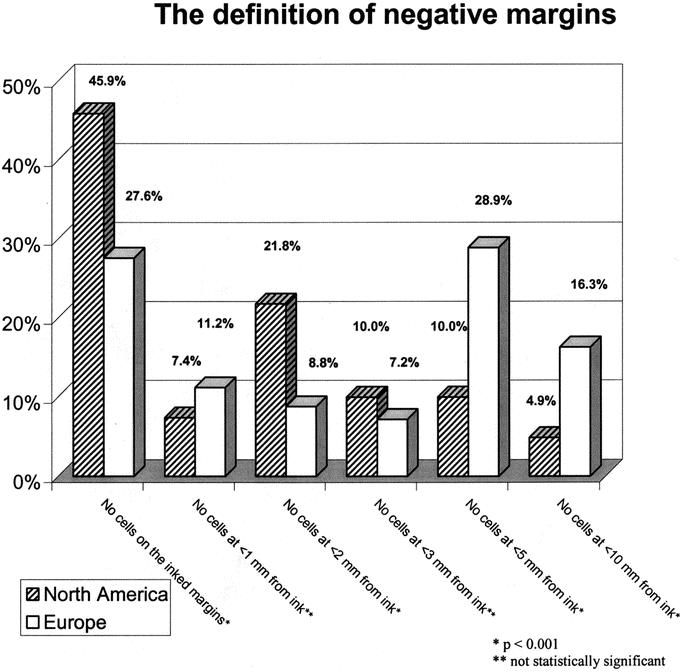
Results: A total of 702 responses were obtained from NA and 431 from Europe to the initial survey. An additional 130 responses were obtained from the United States to the second survey regarding reexcision recommendations. Nearly 46% of the North American respondents required only that there be "no tumor cells on the ink" to deem a margin negative (National Surgical Adjuvant Breast and Bowel Project definition). A total of 7.4% and 21.8% required no tumor cells seen at <1 mm and <2 mm, respectively. The corresponding numbers from European respondents were 27.6%, 11.2%, and 8.8%, respectively (P <0.001). Europeans more frequently required a larger distance (>5 mm) between tumor cells and the inked edges before considering a margin to be negative.
Conclusion: This study revealed significant variation in the perception of negative and close margins among radiation oncologists in NA and Europe. Given these findings, a universal definition of negative margins and consistent recommendations for reexcision are needed.
Figures

Comment in
-
Cost implications of the SSO-ASTRO consensus guideline on margins for breast-conserving surgery with whole breast irradiation in stage I and II invasive breast cancer.Ann Surg Oncol. 2014 May;21(5):1512-4. doi: 10.1245/s10434-014-3605-x. Epub 2014 Feb 28. Ann Surg Oncol. 2014. PMID: 24577813 No abstract available.
References
-
- National Institutes of Health Consensus Development Panel Consensus Statement. Treatment of early-stage breast cancer. J Natl Cancer Inst Monogr. 1992;11:11–15. - PubMed
-
- Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347:1233–1241. - PubMed
-
- Jacobson J, Danforth D, Cowan K, et al. Ten-year results of the National Cancer Institute's randomized trial of breast conservation versus mastectomy for stage I and II breast cancer. N Engl J Med. 1995;332:907–911. - PubMed
-
- van Dongen J, Voogd AC, Fentiman IS, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 2000;92:1143–1150. - PubMed
-
- Blichert-Toft M, Rose C, Anderson JA, et al. Danish randomized trial comparing breast conservation therapy with mastectomy: Six years of life table analysis. J Natl Cancer Inst Monogr. 1992;11:19–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
