

Methylphenidate hydrochloride improves cognitive function in patients with advanced cancer and hypoactive delirium: a prospective clinical study
- PMID: 15798785
- PMCID: PMC551162
Methylphenidate hydrochloride improves cognitive function in patients with advanced cancer and hypoactive delirium: a prospective clinical study
Abstract
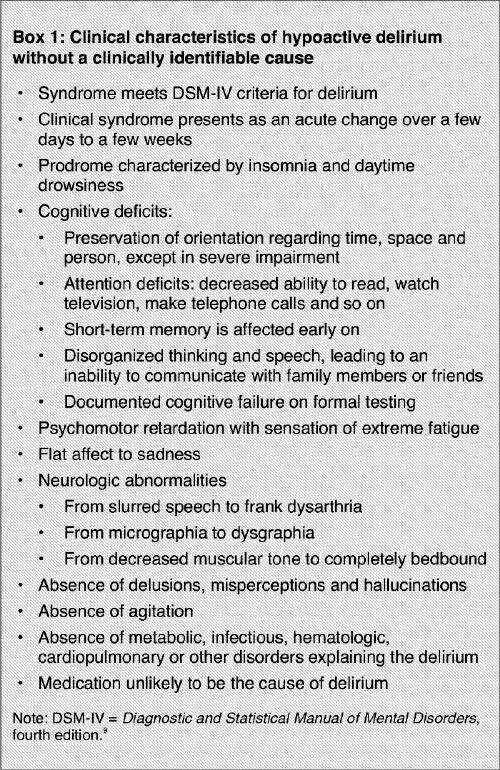
Objective: To investigate the clinical improvement observed in patients with advanced cancer and hypoactive delirium after the administration of methylphenidate hydrochloride.
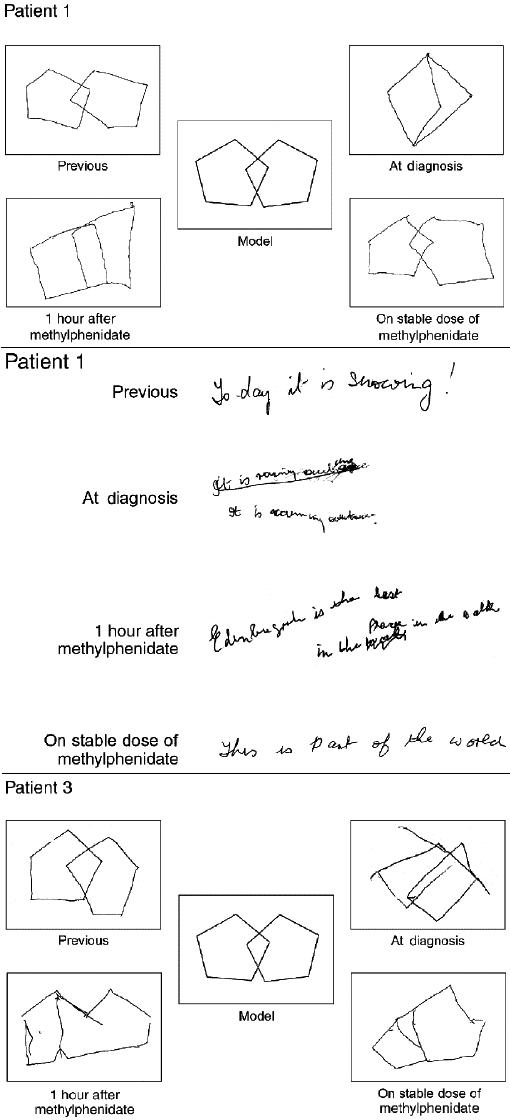
Methods: Fourteen patients with advanced cancer and hypoactive delirium were seen between March 1999 and August 2000 at the Palliative Care Day Hospital and the inpatient Tertiary Palliative Care Unit of Montreal General Hospital, Montreal. They were chosen for inclusion in a prospective clinical study on the basis of (1) cognitive failure documented by the Mini-Mental State Examination (MMSE), (2) sleep-wake pattern disturbances, (3) psychomotor retardation, (4) absence of delusions or hallucinations, and (5) absence of an underlying cause to explain the delirium. All patients were treated with methylphenidate, and changes in their cognitive function were measured using the MMSE.
Results: All 14 patients showed improvement in their cognitive function as documented by the MMSE. The median pretreatment MMSE score (maximum score 30) was 21 (mean 20.9, standard deviation [SD] 4.9), which improved to a median of 27 (mean 24.9, SD 4.7) after the first dose of methylphenidate (p < 0.001, matched, paired Wilcoxon signed rank test). One patient died before reaching a stable dose of methylphenidate. In the other 13 patients, the median MMSE score further improved to 28 (mean 27.8, SD 2.4) (p = 0.02 compared with the median MMSE score documented 1 hour after the first dose of methylphenidate). All patients showed an improvement in psychomotor activities.
Conclusions: Hypoactive delirium that cannot be explained by an underlying cause (metabolic or drug-induced) in patients with advanced cancer appears to be a specific syndrome that could be improved by the administration of methylphenidate.
Objectif: Étudier l'amélioration clinique observée après l'administration de chlorhydrate de méthylphénidate (méthylphénidate) chez des patients atteints de cancer au stade avancé et présentant un délire hypoactif.
Méthodes: Entre mars 1999 et août 2000, à un hôpital de jour en soins palliatifs et l'unit d'hospitalisation en soins palliatifs, Montreal General Hospital, Montréal, on a examiné 14 patients atteints de cancer au stade avancé et présentant un délire hypoactif. On a choisi ces patients pour les inclure dans une étude clinique prospective en fonction (1) de la défaillance de la cognition documentée par le mini-examen de l'état mental (MEEM), (2) des troubles du cycle veille-sommeil, (3) du retard psychomoteur, (4) de l'absence d'illusions ou d'hallucinations et (5) de l'absence de cause sous-jacente pour expliquer le délire. Tous les patients ont été traités au méthylphénidate, et l'on a mesuré les changements de leur fonction cognitive au moyen du MEEM.
Résultats: Les 14 patients ont montré une amélioration de la fonction cognitive documentée par le MEEM. Le résultat médian de l'administration du MEEM avant le traitement (résultat maximal de 30) s'est établi à 21 (moyenne de 20,9, écart type [ET] de 4,9), et s'est amélioré pour atteindre une médiane de 27 (moyenne de 24,9, ET de 4,7) après la première dose de méthylphénidate (p < 0,001, test de Wilcoxon pour observations appariées). Un patient est mort avant qu'on atteigne une dose stable de méthylphénidate. Chez les 13 autres patients, le résultat médian au MEEM s'est amélioré encore pour atteindre 28 (moyenne de 27,8, ET de 2,4) (p = 0,02 comparativement au résultat médian obtenu au MEEM documenté une heure après l'administration de la première dose de méthylphénidate). Tous les patients ont montré une amélioration des activités psychomotrices.
Conclusions: Le délire hypoactif qu'il est impossible d'expliquer par une cause sous-jacente (métabolique ou d'origine médicamenteuse) chez les patients atteints de cancer au stade avancé semble constituer un syndrome spécifique que pourrait améliorer l'administration de méthylphénidate.
Figures
Similar articles
-
The frequency and clinical course of cognitive impairment in patients with terminal cancer.Cancer. 1997 Feb 15;79(4):835-42. Cancer. 1997. PMID: 9024722
-
Clinical utility, factor analysis, and further validation of the memorial delirium assessment scale in patients with advanced cancer: Assessing delirium in advanced cancer.Cancer. 2000 Jun 15;88(12):2859-67. Cancer. 2000. PMID: 10870073
-
[The treatment with methylphenidate of demoralisation, apathy and hypoactive delirium in patients with somatic illness].Ned Tijdschr Geneeskd. 2004 Aug 28;148(35):1738-41. Ned Tijdschr Geneeskd. 2004. PMID: 15468905 Dutch.
-
[Using psychostimulants in end-of-life patients with hypoactive delirium and cognitive disorders: A literature review].Can J Psychiatry. 2010 Jun;55(6):386-93. doi: 10.1177/070674371005500608. Can J Psychiatry. 2010. PMID: 20540834 Review. French.
-
Methylphenidate: established and expanding roles in symptom management.Am J Hosp Palliat Care. 2012 Sep;29(6):483-90. doi: 10.1177/1049909111427029. Epub 2011 Dec 4. Am J Hosp Palliat Care. 2012. PMID: 22144657 Review.
Cited by
-
Methylphenidate as a Novel Adjunct in Opioid-Taking Patients: Insights into Dopaminergic Neuroadaptation and Hypoactive Delirium.Brain Sci. 2025 Aug 8;15(8):850. doi: 10.3390/brainsci15080850. Brain Sci. 2025. PMID: 40867181 Free PMC article. Review.
-
Cognitive impairment after cytotoxic chemotherapy.Neurooncol Pract. 2020 Jan;7(1):11-21. doi: 10.1093/nop/npz052. Epub 2019 Nov 4. Neurooncol Pract. 2020. PMID: 32257280 Free PMC article. Review.
-
A randomized trial on the efficacy of methylphenidate and modafinil for improving cognitive functioning and symptoms in patients with a primary brain tumor.J Neurooncol. 2012 Mar;107(1):165-74. doi: 10.1007/s11060-011-0723-1. Epub 2011 Oct 2. J Neurooncol. 2012. PMID: 21964738 Clinical Trial.
-
Psychopharmacology in cancer.Curr Psychiatry Rep. 2015 Jan;17(1):529. doi: 10.1007/s11920-014-0529-x. Curr Psychiatry Rep. 2015. PMID: 25417593 Review.
-
Acknowledging the relevance of cognitive changes in cancer patients: perspectives of oncology practitioners in Asia.J Cancer Surviv. 2013 Mar;7(1):146-54. doi: 10.1007/s11764-012-0256-4. Epub 2013 Feb 8. J Cancer Surviv. 2013. PMID: 23392850
References
-
- Lawlor PG, Gagnon B, Mancini IL, Pereira JL, Hanson J, Suarez-Almazor ME, et al. Occurrence, causes, and outcome of delirium in patients with advanced cancer: a prospective study. Arch Intern Med 2000;160(6):786-94. - PubMed
-
- Gagnon P, Allard P, Masse B, DeSerres M. Delirium in terminal cancer: a prospective study using daily screening, early diagnosis, and continuous monitoring. J Pain Symptom Manage 2000;19(6):412-26. - PubMed
-
- Lipowski ZJ. Delirium in the elderly patient. N Engl J Med 1989; 320(9):578-82. - PubMed
-
- Weitzner MA, Meyers CA, Valentine AD. Methylphenidate in the treatment of neurobehavioral slowing associated with cancer and cancer treatment. J Neuropsychiatry Clin Neurosci 1995;7(3):347-50. - PubMed
-
- Morita T, Otani H, Tsunoda J, Inoue S, Chihara S. Successful palliation of hypoactive delirium due to multi-organ failure by oral methylphenidate. Support Care Cancer 2000;8(2):134-7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical