

Handheld computer-based decision support reduces patient length of stay and antibiotic prescribing in critical care
- PMID: 15802478
- PMCID: PMC1174884
- DOI: 10.1197/jamia.M1798
Handheld computer-based decision support reduces patient length of stay and antibiotic prescribing in critical care
Abstract
Objective: This study assessed the effect of a handheld computer-based decision support system (DSS) on antibiotic use and patient outcomes in a critical care unit.
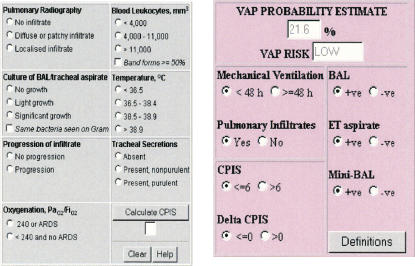
Design: A DSS containing four types of evidence (patient microbiology reports, local antibiotic guidelines, unit-specific antibiotic susceptibility data for common bacterial pathogens, and a clinical pulmonary infection score calculator) was developed and implemented on a handheld computer for use in the intensive care unit at a tertiary referral hospital. System impact was assessed in a prospective "before/after" cohort trial lasting 12 months. Outcome measures were defined daily doses (DDDs) of antibiotics per 1,000 patient-days, patient length of stay, and mortality.
Results: The number of admissions, APACHE (Acute Physiology, Age, and Chronic Health Evaluation) II and SAPS (Simplified Acute Physiology Score) II for patients in preintervention, and intervention (DSS use) periods were statistically comparable. The mean patient length of stay and the use of antibiotics in the unit during six months of the DSS use decreased from 7.15 to 6.22 bed-days (p = 0.02) and from 1,767 DDD to 1,458 DDD per 1,000 patient-days (p = 0.04), respectively, with no change in mortality. The DSS was accessed 674 times during 168 days of the trial. Microbiology reports and antibiotic guidelines were the two most commonly used (53% and 22.5%, respectively) types of evidence. The greatest reduction was observed in the use of beta-lactamase-resistant penicillins and vancomycin.
Conclusion: Handheld computer-based decision support contributed to a significant reduction in patient length of stay and antibiotic prescribing in a critical care unit.
Figures

References
-
- Evans RS, Pestotnik SL, Classen DC, Clemmer TP, Weaver LK, Orme JF Jr, et al. A computer-assisted management program for antibiotics and other antiinfective agents. N Engl J Med. 1998;338:232–8. - PubMed
-
- Hunt DL, Haynes RB, Hanna SE, Smith K. Effects of computer-based clinical decision-support systems on physician performance and patient outcomes: a systematic review. JAMA. 1998;280:1339–46. - PubMed
-
- Miller SM, Beattie MM, Butt AA. Personal digital assistant infectious diseases applications for health care professionals. Clin Infect Dis. 2003;36:1018–29. - PubMed
-
- Beasley BW. Utility of palmtop computers in a residency program: a pilot study. South Med J. 2002;95:207–11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
