

Kidney transplantation under minimal immunosuppression after pretransplant lymphoid depletion with Thymoglobulin or Campath
- PMID: 15804464
- PMCID: PMC2980295
- DOI: 10.1016/j.jamcollsurg.2004.12.024
Kidney transplantation under minimal immunosuppression after pretransplant lymphoid depletion with Thymoglobulin or Campath
Abstract
Background: Multiple drug immunosuppression has allowed the near elimination of rejection, but without commensurate improvements in longterm graft survival and at the cost of quality of life. We have suggested that transplantation outcomes can be improved by modifying the timing and dosage of immunosuppression to facilitate natural mechanisms of alloengraftment and acquired tolerance.
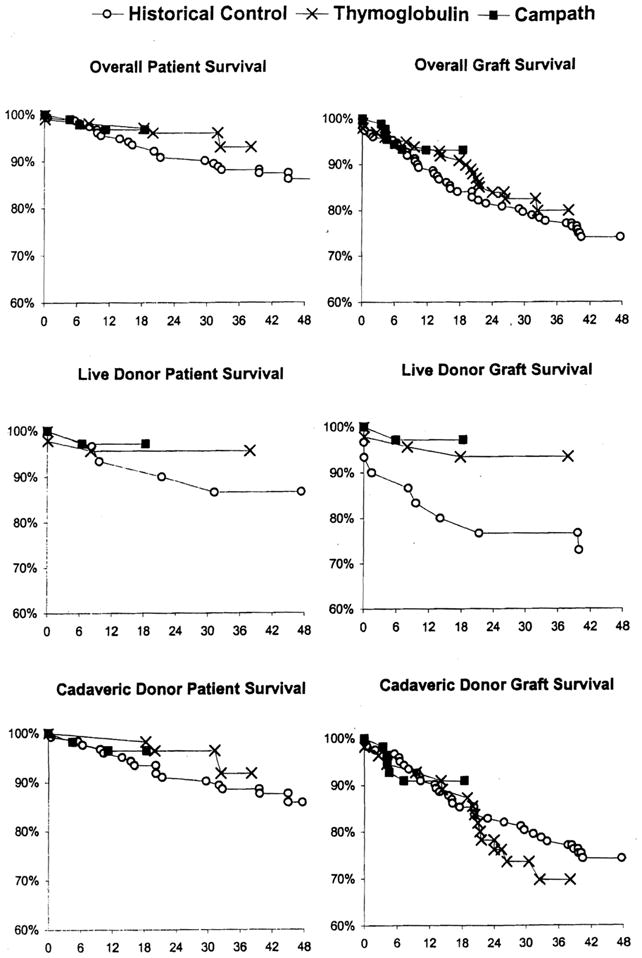
Study design: Two therapeutic principles were applied for kidney transplantation: pretransplant recipient conditioning with antilymphoid antibody preparations (Thymoglobulin [Sangstat] or Campath [ILEX Pharmaceuticals]), and minimal posttransplant immunosuppression with tacrolimus monotherapy including "spaced weaning" of maintenance doses when possible. The results in Thymoglobulin- (n = 101) and Campath-pretreated renal transplantation recipients (n = 90) were compared with those in 152 conventionally immunosuppressed recipients in the immediately preceding era.
Results: Spaced weaning was attempted in more than 90% of the kidney transplant recipients after pretreatment with both lymphoid-depleting agents, and is currently in effect in two-thirds of the survivors. Although there was a much higher rate of acute rejection in the Thymoglobulin-pretreated recipients than in either the Campath-pretreated or historic control recipients, patient and graft survival in both lymphoid depletion groups is at least equivalent to that of historic control patients. In the Thymoglobulin-conditioned patients for whom followups are now 24 to 40 months, chronic allograft nephropathy (CAN) progressed at the same rate as in historic control patients. Selected patients on weaning developed donor-specific nonreactivity.
Conclusions: After lymphoid depletion, kidney transplantation can be readily accomplished under minimal immunosuppression with less dependence on late maintenance immunosuppression and a better quality of life. Campath was the more effective agent for pretreatment. Guidelines for spaced weaning need additional refinement.
Conflict of interest statement
No competing Interests declared.
Figures


References
-
- Starzl TE, Porter KA, Iwasaki Y, et al. The use of antilymphocyte globulin in human renal homotransplantation. In: Wolstenholme GEW, O’Connor M, editors. Antilymphocytic Serum. London: J and A Churchill Limited; 1967. pp. 4–34.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
