

Corticosteroid injections for painful shoulder: a meta-analysis
- PMID: 15808040
- PMCID: PMC1463095
Corticosteroid injections for painful shoulder: a meta-analysis
Abstract
Background: There are no systematic reviews of corticosteroids for shoulder pain that calculate the numbers needed to treat.
Aim: We wished to determine the effectiveness in terms of improvement of symptoms of intra-articular and subacromial injections of corticosteroid for rotator cuff tendonitis and frozen shoulder.
Design of study: Systematic review and meta-analysis of randomised controlled trials.
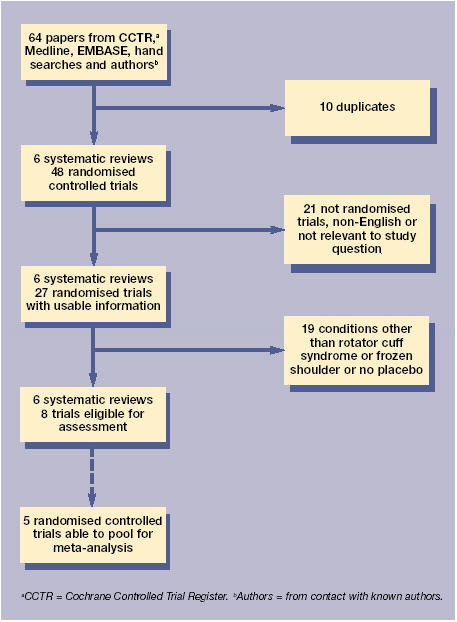
Method: Data sources included the Cochrane Controlled Trials Register, Medline, EMBASE, hand searches and author contacts. The review methods required any randomised controlled trial in which the effectiveness of subacromial or intra-articular steroid injections versus placebo and versus non-steroidal anti-inflammatory medication, could be ascertained. The outcome was improvement of symptoms. The data abstraction was done independently, as was the validity assessment. The data was pooled using Review Manager 4.1.
Results: Seven studies were reviewed for corticosteroids versus placebo and three for corticosteroids versus nonsteroidal anti-inflammatory drugs (NSAIDs). The relative risk for improvement for subacromial corticosteroid injection for rotator cuff tendonitis was 3.08 (95% confidence interval [CI] = 1.94 to 4.87). The number needed to treat based on the pooled relative risk was 3.3 (95% CI = 1.8 to 7.7) patients to obtain one improvement. The relative risk for high dose (50 mg of prednisone or more) was 5.9 (95% CI = 2.8 to 12.6). The relative risk for improvement with steroids compared with NSAIDs was 1.43 (95% CI = 0.95 to 2.16). The number needed to treat for corticosteroids versus NSAIDs was 2.5 (95% CI = 1 to 9) for one significant study. The relative risks for intra-articular steroid injection for rotator cuff tendonitis were not statistically significant.
Conclusion: Subacromial injections of corticosteroids are effective for improvement for rotator cuff tendonitis up to a 9-month period. They are also probably more effective than NSAID medication. Higher doses may be better than lower doses for subacromial corticosteroid injection for rotator cuff tendonitis.
Figures
Comment in
-
Corticosteroid injections: from bench to bedside?Br J Gen Pract. 2005 Apr;55(513):314. Br J Gen Pract. 2005. PMID: 15826442 Free PMC article. No abstract available.
References
-
- Palmer KT, Cooper C, Walker-Bone K, et al. Use of keyboards and symptoms in the neck and arm: evidence from a national survey. Occup Med (Lond) 2001;5:392–395. - PubMed
-
- Green S, Buchbinder R, Glazier R, Forbes A. Interventions for shoulder pain: systematic review. Cochrane Musculoskeletal Group Cochrane Database of Systematic Reviews. 2002:3. - PubMed
-
- McQuay HJ, Moore RA, Eccleston C, et al. Systematic review of outpatient services for chronic pain control. Health Technol Assess. 1997;1:i–iv. 1–135. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials