

Value of CT in the diagnosis and management of gallstone ileus
- PMID: 15810081
- PMCID: PMC4305784
- DOI: 10.3748/wjg.v11.i14.2142
Value of CT in the diagnosis and management of gallstone ileus
Abstract
Aim: To retrospectively establish the diagnostic criteria of gallstone ileus on CT, and to prospectively apply these criteria to determine the diagnostic accuracy of CT to confirm or exclude gallstone ileus in patients who presented with acute small bowel obstruction (SBO). Another purpose was to ascertain whether the size of ectopic gallstones would affect treatment strategy.
Methods: Fourteen CT scans in cases of proved gallstone ileus were evaluated retrospectively by two radiologists for the presence or absence of previously reported CT findings to establish the diagnostic criteria. These criteria were applied in a prospective contrast enhanced CT study of 165 patients with acute SBO, which included those 14 cases of gallstone ileus. The hard copy images of 165 CT studies were reviewed by a different group of two radiologists but without previous knowledge of the patient's final diagnosis. All CT data were further analyzed to determine the diagnostic accuracy of gallstone ileus when using CT in prospective evaluation of acute SBO. The size of ectopic gallstone on CT was correlated with the clinical course.
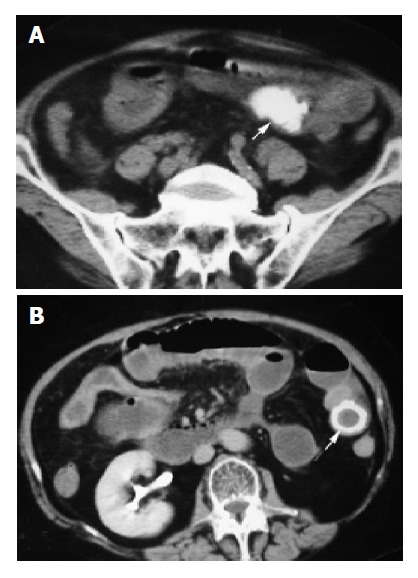
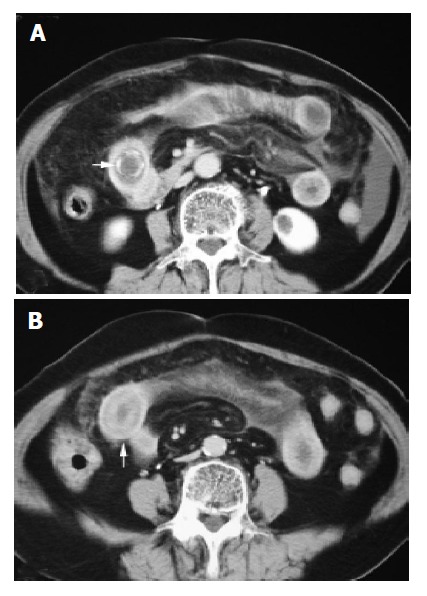
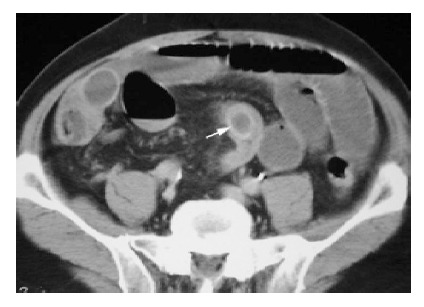
Results: The diagnostic criteria of gallstone ileus on CT were established retrospectively, which included: (1) SBO; (2) ectopic gallstone; either rim-calcified or total-calcified; (3) abnormal gall bladder with complete air collection, presence of air-fluid level, or fluid accumulation with irregular wall. Prospectively, CT confirmed the diagnosis in 13 cases of gallstone ileus with these three criteria. Only one false negative case could be identified. The remaining 151 patients are true negative cases and no false positive case could be disclosed. The overall sensitivity, specificity and accuracy of CT in diagnosing gallstone ileus were 93%, 100%; and 99%, respectively. Surgical exploration was performed in 13 patients of gallstone ileus with ectopic stones sized larger than 3 cm. One patient recovered uneventfully following conservative treatment with an ectopic stone sized 2 cm in the long axis.
Conclusion: Contrast enhanced CT imaging offered crucial evidence not only for the diagnosis of gallstone ileus but also for decision making in management strategy.
Figures



References
-
- Hudspeth AS, McGuirt WF. Gallstone ileus. A continuing surgical problem. Arch Surg. 1970;100:668–672. - PubMed
-
- Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. Br J Surg. 1990;77:737–742. - PubMed
-
- Maglinte DD, Reyes BL, Harmon BH, Kelvin FM, Turner WW, Hage JE, Ng AC, Chua GT, Gage SN. Reliability and role of plain film radiography and CT in the diagnosis of small-bowel obstruction. AJR Am J Roentgenol. 1996;167:1451–1455. - PubMed
-
- Shrake PD, Rex DK, Lappas JC, Maglinte DD. Radiographic evaluation of suspected small bowel obstruction. Am J Gastroenterol. 1991;86:175–178. - PubMed
-
- Lasson A, Lorén I, Nilsson A, Nirhov N, Nilsson P. Ultrasonography in gallstone ileus: a diagnostic challenge. Eur J Surg. 1995;161:259–263. - PubMed
