

Annulling a dangerous liaison: vaccination strategies against AIDS and tuberculosis
- PMID: 15812488
- PMCID: PMC7095892
- DOI: 10.1038/nm1221
Annulling a dangerous liaison: vaccination strategies against AIDS and tuberculosis
Erratum in
- Nat Med. 2005 May;11(5):578
Abstract
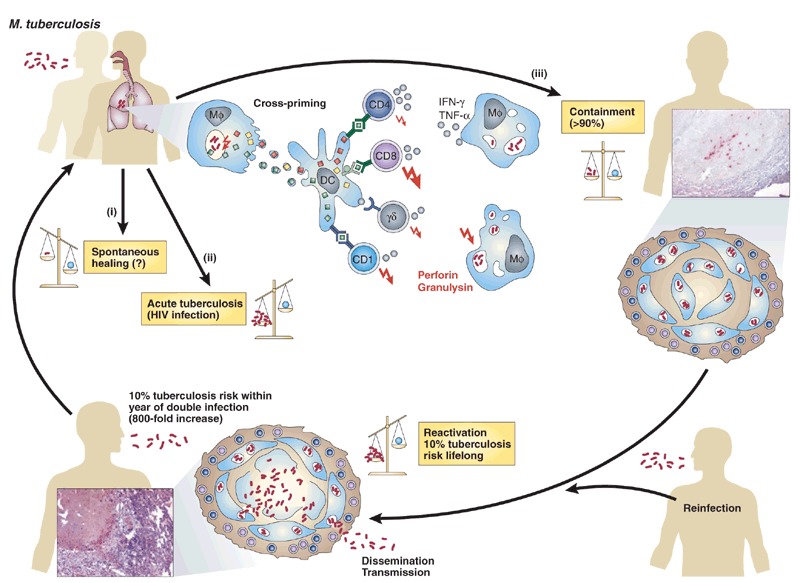
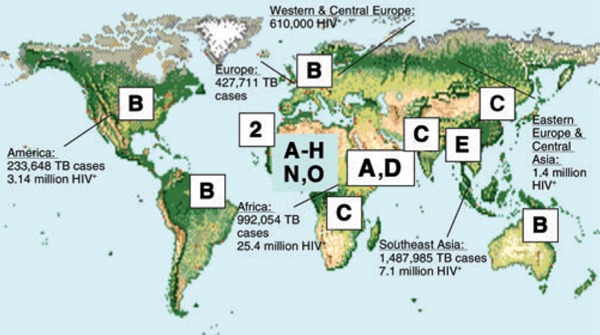
Human immunodeficiency virus (HIV) and Mycobacterium tuberculosis annually cause 3 million and 2 million deaths, respectively. Last year, 600,000 individuals, doubly infected with HIV and M. tuberculosis, died. Since World War I, approximately 150 million people have succumbed to these two infections--more total deaths than in all wars in the last 2,000 years. Although the perceived threats of new infections such as SARS, new variant Creutzfeldt-Jakob disease and anthrax are real, these outbreaks have caused less than 1,000 deaths globally, a death toll AIDS and tuberculosis exact every 2 h. In 2003, 40 million people were infected with HIV, 2 billion with M. tuberculosis, and 15 million with both. Last year, 5 million and 50 million were newly infected with HIV or M. tuberculosis, respectively, with 2 million new double infections. Better control measures are urgently needed.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- World Health Organization. Global Tuberculosis Control: Surveillance, Planning, Financing (World Health Organization, Geneva, 2004).
-
- Calmette A. Die Schutzimpfung gegen Tuberkulose mit “BCG”. 1928.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
