

Preangiographic evaluation of spinal dural arteriovenous fistulas with elliptic centric contrast-enhanced MR Angiography and effect on radiation dose and volume of iodinated contrast material
- PMID: 15814910
- PMCID: PMC7977123
Preangiographic evaluation of spinal dural arteriovenous fistulas with elliptic centric contrast-enhanced MR Angiography and effect on radiation dose and volume of iodinated contrast material
Abstract
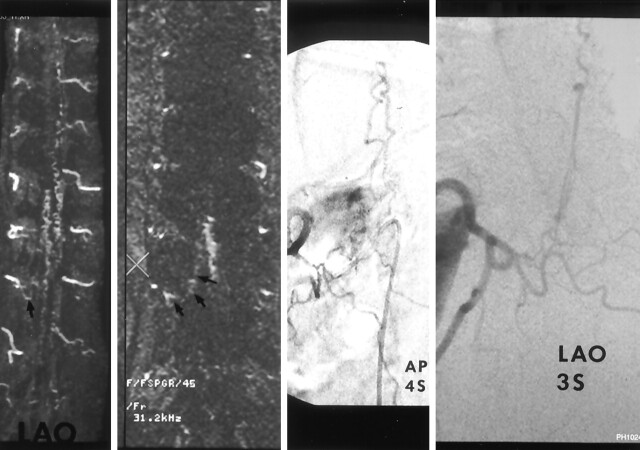
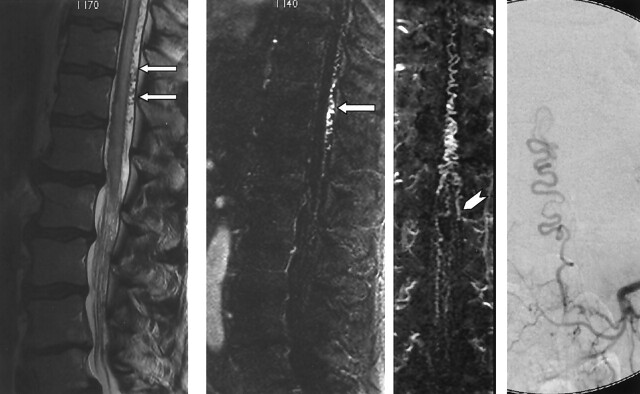
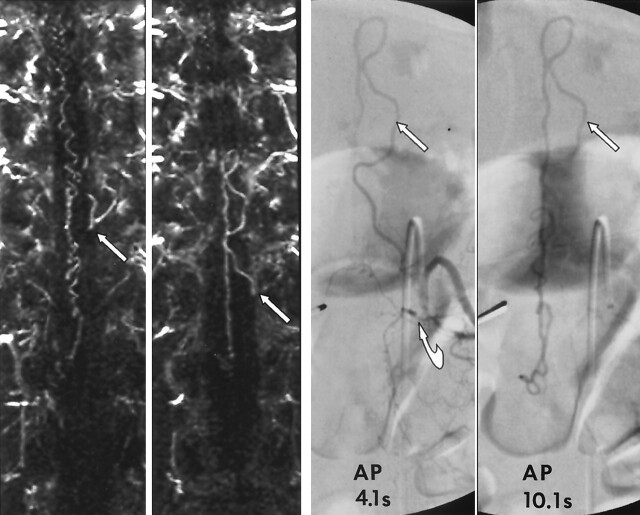
Background and purpose: The detection and localization of spinal dural arteriovenous fistulas (AVFs) remain diagnostic challenges. This study tested the hypothesis that elliptic centric contrast-enhanced MR angiography (MRA) can be used to detect spinal dural AVFs, predict the level of fistulas, and reduce the radiation dose and volume of iodinated contrast material associated with conventional angiography.
Methods: We examined 31 patients who presented with suspected spinal dural AVF between December 2000 and March 2004. All patients underwent MRA and conventional angiography. The effect of MRA on subsequent conventional angiography was assessed by analyzing total fluoroscopy time and volume of iodinated contrast material used.
Results: At angiography, spinal dural AVFs were diagnosed in 22 of 31 patients, and MRA depicted an AVF in 20 of the 22 patients. MRA findings correctly predicted a negative angiogram in seven of nine cases. Of the 20 true-positive MRA results, the level of the fistula was included in the imaging volume in 14. In 13 of these 14 cases, MRA results correctly predicted the side and the level of the fistula to within one vertebral level. Fluoroscopy time and the volume of contrast agent was reduced by more than 50% in the 13 patients with a spinal dural AVF in whom MRA prospectively indicated the correct level.
Conclusion: Contrast-enhanced MRA can be used to detect spinal dural AVFs, predict the level of fistulas, and substantially reduce the radiation dose and volume of contrast agent associated with catheter spinal angiography.
Figures

References
-
- Farb RI, Kim JK, Willinsky RA, et al. Spinal dural arteriovenous fistula localization with a technique of first-pass gadolinium-enhanced MR angiography: initial experience. Radiology 2002;222:843–850 - PubMed
-
- Anson JA, Spetzler RF. Classification of spinal arteriovenous malformations and implications for treatment. BNI Qtr 1992;8:2–8
-
- Grote EH, Bien S. Arteriovenous malformations of the spinal cord. In: Youmans JR, ed. Neurological Surgery. 4th ed. Philadelphia: W.B. Saunders;1996. :1511–1530
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources