

PC VIPR: a high-speed 3D phase-contrast method for flow quantification and high-resolution angiography
- PMID: 15814915
- PMCID: PMC7977085
PC VIPR: a high-speed 3D phase-contrast method for flow quantification and high-resolution angiography
Abstract
Background and purpose: Three-dimensional phase-contrast (3DPC) is limited by long imaging times, limited coverage, flow artifacts, and the need to perform multiple additional 2D examinations (2DPC) to measure flow. A highly undersampled 3D radial acquisition (isotropic-voxel radial projection imaging [PCVIPR]) makes it possible to increase the product of volume coverage and spatial resolution by a factor of 30 for the same imaging time as conventional Cartesian 3DPC. This provides anatomic information over a large volume with high isotropic resolution and permits retrospective measurement of average flow rates throughout the volume.
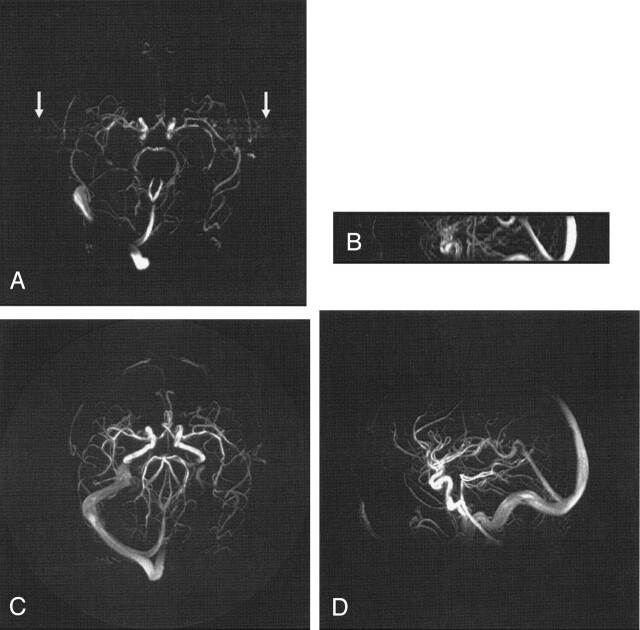
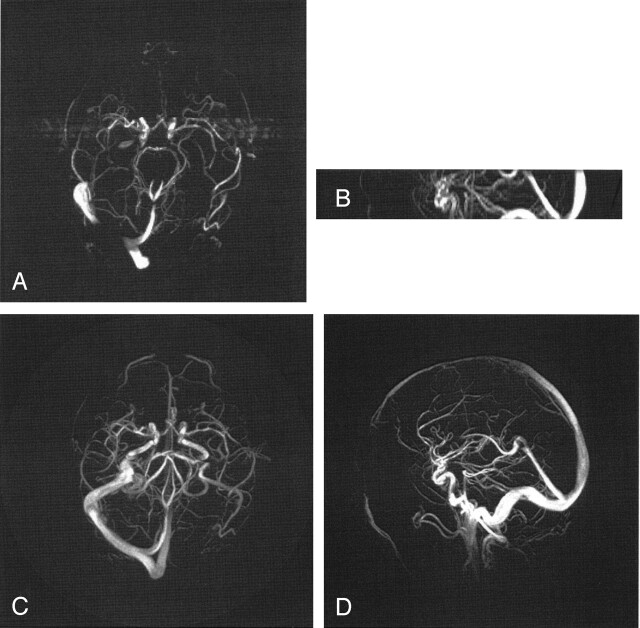
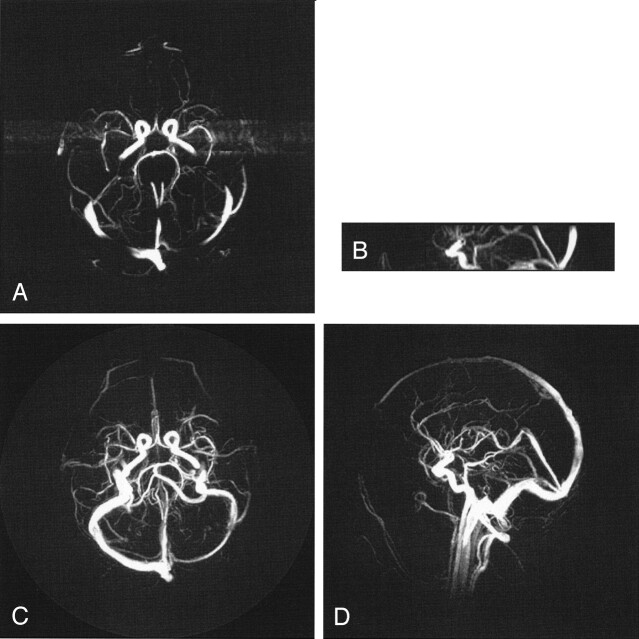
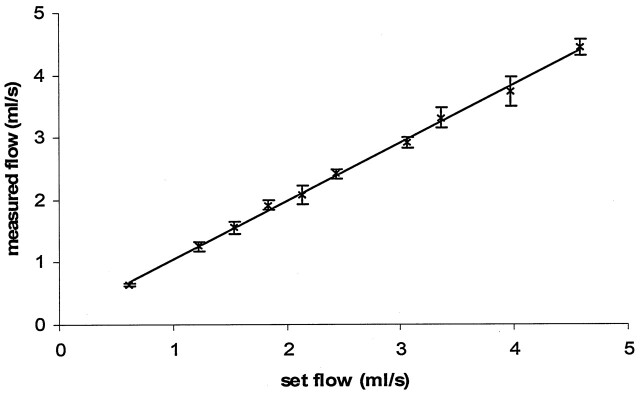
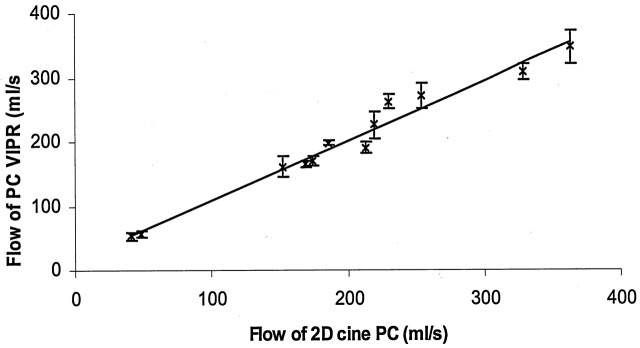
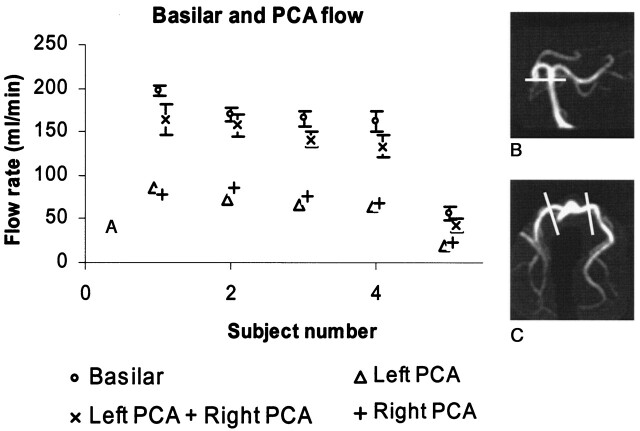
Methods: PCVIPR acquires a reference and three flow-encoded acquisitions for each VIPR projection. Complex difference images were formed by combining information from all flow directions. Following retrospective definition of planes perpendicular to selected vessels, volume flow rates were determined by using phase-difference information. The accuracy of average flow measurement was investigated in a phantom and in six volunteers. Anatomic PCVIPR images acquired in three patients and three volunteers by using a 384(3) matrix were compared with conventional Cartesian 3DPC.
Results: The flow validation produced R2 = 0.99 in vitro and R2 = 0.97 in vivo. PCVIPR produced minimal streak and pulsatile flow artifacts. PCVIPR produced far higher resolution and volume coverage in comparable imaging times. The highest acceleration factors relative to 3DPC were achieved by using gadolinium-contrast material. Ultimately, acceleration factors are limited by signal-to-noise ratio.
Conclusion: PCVIPR rapidly provides isotropic high-resolution angiographic images and permits retrospective measurement of average flow rate throughout the volume without the need to prescribe multiple 2D acquisition planes.
Figures
References
-
- Dumoulin CL, Souza SP, Walker MF, Wagle W. Three-dimensional phase contrast angiography. Magn Reson Med 1989;9:139–149 - PubMed
-
- Block WF, Barger AV, Mistretta CA. Vastly undersampled isotropic projection imaging. In: Proceedings of the Eighth International Society for Magnetic Resonance in Medicine, Denver, CO. April 1–7, 2000. :161
-
- Barger AV, Block WF, Toropov Y, Grist TM, Mistretta CA. Time-resolved contrast-enhanced imaging with isotropic resolution and broad coverage using a undersampling 3D projection trajectory. Magn Reson Med 2002;48:297–305 - PubMed
-
- Wong STS, Roos MS. Strategy for sampling on a sphere with applications to 3D selective pulse design. In: Proceedings of 12th meeting of the Society of Magnetic Resonance in Medicine, New York, NY. August 14–20,1993. :1178
-
- Peters DC, Korosec FR, Grist TM, et al. Undersampled projection reconstruction applied to MR angiography. Magn Reson Med 2000;43:91–101 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources