

Case Reports
MR Imaging of pial melanosis secondary to a posterior fossa melanotic ependymoma
Affiliations
- PMID: 15814924
- PMCID: PMC7977103
Item in Clipboard
Case Reports
MR Imaging of pial melanosis secondary to a posterior fossa melanotic ependymoma
AJNR Am J Neuroradiol.
2005 Apr.
Abstract
A 36-year-old man presented with trouble speaking and bilateral progressive hearing loss. MR imaging and histopathologic results revealed a posterior fossa melanotic ependymoma. Pial surfaces appeared hyperintense on T1-weighted images and hypointense on T2-weighted images. Histopathologic examination revealed that tumor cells and interstitial spaces had abundant melanin accumulation. There was no evidence of hemosiderin in tumor cells and in interstitial spaces. Pial melanin accumulation secondary to a posterior fossa melanotic ependymoma explained our MR findings.
Figures
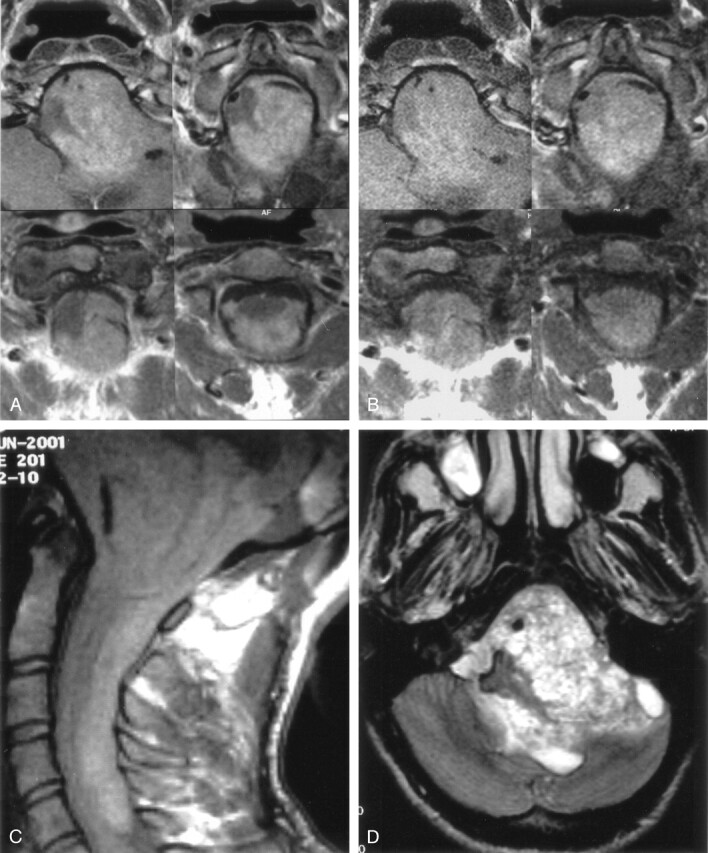
Contrast-enhanced (A) and nonenhanced (B) T1-weighted axial MR images reveal a posterior fossa mass that extends cranially through 4th ventricle and left cerebellopontine cistern and caudally through foramen magnum. Nonenhanced T1-weighted sagittal MR image (C) shows that a hyperintense melanin-containing mass displaces the medulla oblongata and spinal cord and extends down to the level of the 6th cervical vertebra. T2-weighted axial MR image (D) shows a heterogeneous posterior fossa mass.
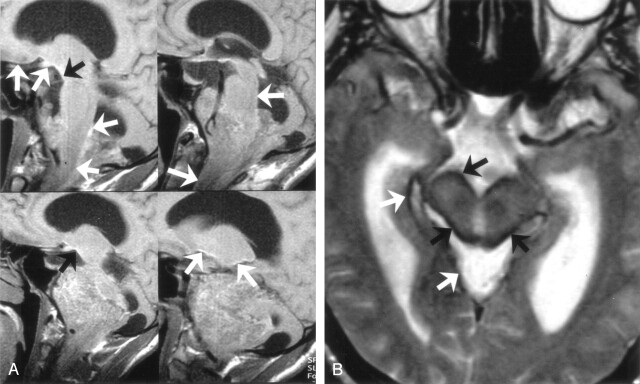
Four sequential T1-weighted nonenhanced sagittal MR images (A) show linear high signal intensity on the pial surfaces of the cerebrum, cerebellum, brain stem, and spinal cord secondary to pial melanin accumulation (arrows). T2-weighted axial MR image (B) shows striking signal intensity voids on the pial surfaces of brain stem (arrows).
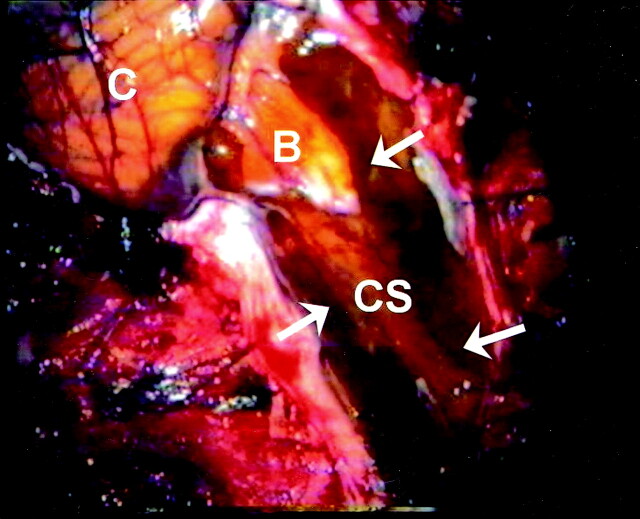
Photograph of the surgery shows diffuse black and dark brown pigmentation of the pial surfaces of medulla oblongata and medulla spinalis (arrows). C indicates cerebellum; B, bulbus; CS, cervical spinal cord.
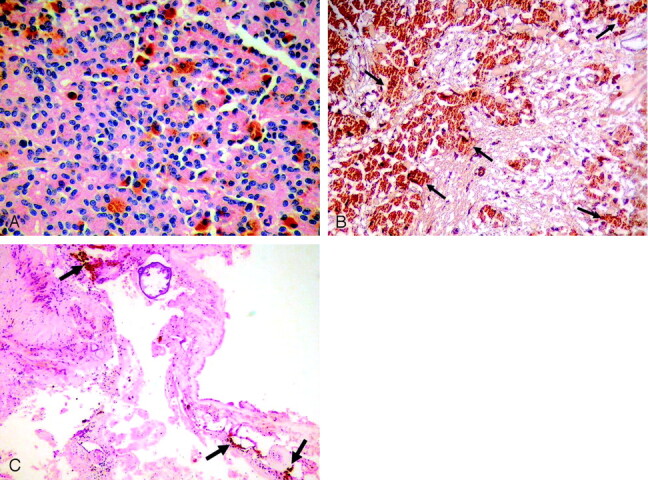
A, Microscopy shows characteristic histopathologic features of ependymoma with true rosettes and pseudorosettes, perivascular orientation (hematoxylin-eosin; original magnification × 200). B, Tumor cells have abundant brown melanin pigment (arrows) in the cytoplasm that shows positivity for Masson-Fontana (original magnification ×100). C, Brown melanin pigment is also present in the interstitial space of the tumor (arrows; hematoxylin-eosin; original magnification ×40).
Similar articles
-
MRI findings in a case of a superficial siderosis associated with an ependymoma.J Neuroradiol. 2002 Jun;29(2):136-8. J Neuroradiol. 2002. PMID: 12297737
-
Secondary superficial siderosis of the central nervous system in a patient presenting with sensorineural hearing loss.Neuroradiology. 1998 May;40(5):312-4. doi: 10.1007/s002340050591. Neuroradiology. 1998. PMID: 9638673
-
Intracranial metastatic melanoma: correlation between MR imaging characteristics and melanin content.AJR Am J Roentgenol. 1995 Dec;165(6):1503-12. doi: 10.2214/ajr.165.6.7484597. AJR Am J Roentgenol. 1995. PMID: 7484597
-
Posterior fossa brain tumors and arterial hypertension.Neurosurg Rev. 2006 Oct;29(4):265-9; discussion 269. doi: 10.1007/s10143-006-0036-6. Epub 2006 Aug 19. Neurosurg Rev. 2006. PMID: 16924459 Review.
-
[Normal and abnormal meningeal enhancement: MRI features].J Radiol. 2005 Nov;86(11):1659-83. doi: 10.1016/s0221-0363(05)81507-0. J Radiol. 2005. PMID: 16269979 Review. French.
Cited by
-
Melanotic choroid plexus carcinoma of the posterior fossa.J Clin Neurol. 2011 Jun;7(2):105-6. doi: 10.3988/jcn.2011.7.2.105. Epub 2011 Jun 28. J Clin Neurol. 2011. PMID: 21779301 Free PMC article.
-
Pigmented ependymoma, a tumor with predilection for the middle-aged adult: case report with methylation classification and review of 16 literature cases.Free Neuropathol. 2022 Jul 8;3:16. doi: 10.17879/freeneuropathology-2022-4076. eCollection 2022 Jan. Free Neuropathol. 2022. PMID: 37284162 Free PMC article.
References
-
- Chan AC, Ho LC, Yip WW, Cheung FC. Pigmented ependymoma with lipofuscin and neuromelanin production. Arch Pathol Lab Med 2003;127:872–875 - PubMed
-
- Kakkar N, Vasishta RK, Banerjee AK. Pathology teach and tell: melanotic ependymoma. Pediatr Pathol Mol Med 2003;22:171–174 - PubMed
-
- McCloskey JJ, Parker JC Jr, Brooks WH, Blacker HM. Melanin as a component of cerebral gliomas: the melanotic cerebral ependymoma. Cancer 1976;37:2373–2379 - PubMed
-
- Rosenblum MK, Erlandson RA, Aleksic SN, Budzilovich GN. Melanotic ependymoma and subependymoma. Am J Surg Pathol 1990;14:729–736 - PubMed
-
- Panyathanya R, Chantarakul N. Melanotic ependymoma with distant metastases. J Med Assoc Thai 1982;65:454–458 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical