

Does socioeconomic status affect mortality subsequent to hospital admission for community acquired pneumonia among older persons?
- PMID: 15819975
- PMCID: PMC1090611
- DOI: 10.1186/1477-5751-4-4
Does socioeconomic status affect mortality subsequent to hospital admission for community acquired pneumonia among older persons?
Abstract
Background: Low socioeconomic status has been associated with increased morbidity and mortality for various health conditions. The purpose of this study was twofold: to examine the mortality experience of older persons admitted to hospital with community acquired pneumonia and to test the hypothesis of whether an association exists between socioeconomic status and mortality subsequent to hospital admission for community-acquired pneumonia.
Methods: A population based retrospective cohort study was conducted including all older persons patients admitted to Ontario hospitals with community acquired pneumonia between April 1995 and March 2001. The main outcome measures were 30 day and 1 year mortality subsequent to hospital admission for community-acquired pneumonia.
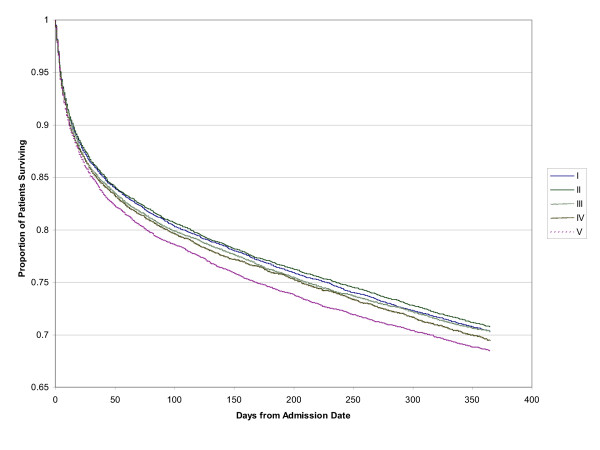
Results: Socioeconomic status for each patient was imputed from median neighbourhood income. Multivariate analyses were undertaken to adjust for age, sex, co-morbid illness, hospital and physician characteristics. The study sample consisted of 60,457 people. Increasing age, male gender and high co-morbidity increased the risk for mortality at 30 days and one year. Female gender and having a family physician as attending physician reduced mortality risk. The adjusted odds of death after 30-days for the quintiles compared to the lowest income quintile (quintile 1) were 1.02 (95% CI: 0.95-1.09) for quintile 2, 1.04 (95% CI: 0.97-1.12) for quintile 3, 1.01 (95% CI: 0.94-1.08) for quintile 4 and 1.03 (95% CI: 0.96-1.12) for the highest income quintile (quintile 5). For 1 year mortality, compared to the lowest income quintile the adjusted odds ratios were 1.01 (95% CI: 0.96-1.06) for quintile 2, 0.99 (95% CI: 0.94-1.04) for quintile 3, 0.99 (95% CI: 0.93-1.05) for quintile 4 and 1.03 (95% CI: 0.97-1.10) for the highest income quintile.
Conclusion: Socioeconomic status is not associated with mortality in the older persons from community-acquired pneumonia in Ontario, Canada.
Figures

Similar articles
-
Development of a prognostic index for 90-day mortality in patients discharged after admission to hospital for community-acquired pneumonia.Thorax. 2009 Jun;64(6):496-501. doi: 10.1136/thx.2008.098814. Epub 2009 Feb 22. Thorax. 2009. PMID: 19237392
-
Association between timing of intensive care unit admission and outcomes for emergency department patients with community-acquired pneumonia.Crit Care Med. 2009 Nov;37(11):2867-74. doi: 10.1097/CCM.0b013e3181b02dbb. Crit Care Med. 2009. PMID: 19770748
-
Arterial carbon dioxide tension on admission as a marker of in-hospital mortality in community-acquired pneumonia.Am J Med. 2005 Feb;118(2):145-50. doi: 10.1016/j.amjmed.2004.10.014. Am J Med. 2005. PMID: 15694899
-
Evidence-based emergency medicine/critically appraised topic. Evidence behind the 4-hour rule for initiation of antibiotic therapy in community-acquired pneumonia.Ann Emerg Med. 2008 May;51(5):651-62, 662.e1-2. doi: 10.1016/j.annemergmed.2007.10.022. Epub 2008 Feb 13. Ann Emerg Med. 2008. PMID: 18272253 Review.
-
The "peripneumonia" period in the older adult.Compr Ther. 1994;20(5):300-5. Compr Ther. 1994. PMID: 8045088 Review.
Cited by
-
Influence of socioeconomic status on community-acquired pneumonia outcomes in elderly patients requiring hospitalization: a multicenter observational study.BMC Public Health. 2010 Jul 15;10:421. doi: 10.1186/1471-2458-10-421. BMC Public Health. 2010. PMID: 20633254 Free PMC article.
-
Psychosocial factors and hospitalisations for COVID-19: Prospective cohort study based on a community sample.Brain Behav Immun. 2020 Oct;89:569-578. doi: 10.1016/j.bbi.2020.06.021. Epub 2020 Jun 17. Brain Behav Immun. 2020. PMID: 32561221 Free PMC article.
-
Host and environmental determinants of in-hospital mortality in community-acquired pneumonia: evidence of seasonality, socioeconomic factors, and hospital differentiation in Portugal.BMC Pulm Med. 2025 Jun 3;25(1):278. doi: 10.1186/s12890-025-03716-8. BMC Pulm Med. 2025. PMID: 40462005 Free PMC article.
-
Education and pneumonia mortality: a trend analysis of its inequalities in Colombian adults.BMJ Open Respir Res. 2020 Nov;7(1):e000695. doi: 10.1136/bmjresp-2020-000695. BMJ Open Respir Res. 2020. PMID: 33199401 Free PMC article.
-
Comparative study of virulence potential, phylogenetic origin, CRISPR-Cas regions and drug resistance of Escherichia coli isolates from urine and other clinical materials.Front Microbiol. 2023 Nov 29;14:1289683. doi: 10.3389/fmicb.2023.1289683. eCollection 2023. Front Microbiol. 2023. PMID: 38094634 Free PMC article.
References
-
- Kaplan V, Angus DC, Griffin MF, Clermont G, Scott Watson R, Linde-Zwirble WT. Hospitalized community-acquired pneumonia in the older persons: age- and sex-related patterns of care and outcome in the United States. Am J Respir Crit Care Med. 2002;165:766–772. - PubMed
-
- Health Canada. Respiratory Disease in Canada. Ottawa, Canada; 2001. Chapter 7: Infectious Diseases.
-
- Evans RG, Barer M, Marmor T. Why Are Some People Healthy and Others Not? The Determinants of Health in Populations. New York: Aldine de Gruyter; 1994.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
