

Epidemiology and management of heart failure and left ventricular systolic dysfunction in the aftermath of a myocardial infarction
- PMID: 15831613
- PMCID: PMC1876349
- DOI: 10.1136/hrt.2005.062026
Epidemiology and management of heart failure and left ventricular systolic dysfunction in the aftermath of a myocardial infarction
Abstract
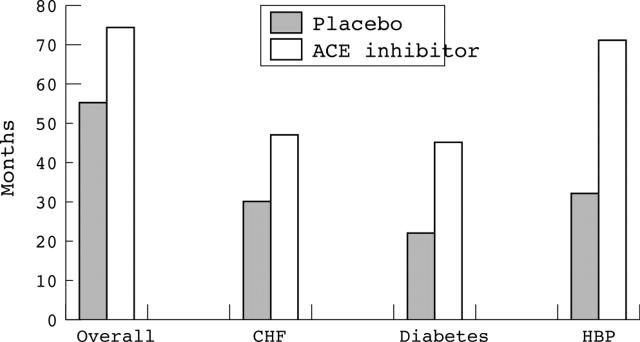
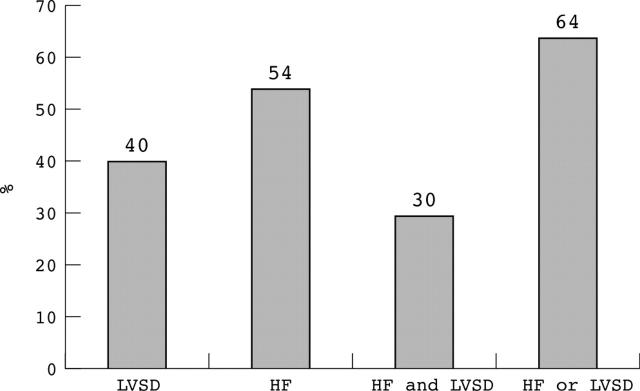
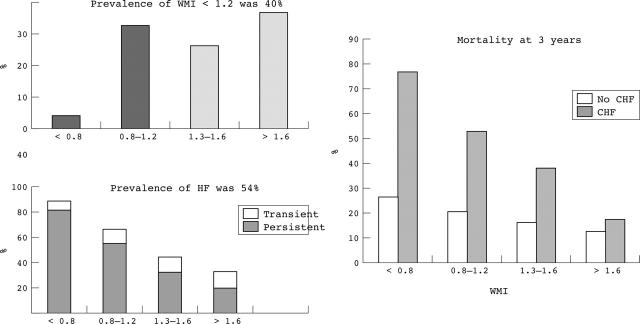
Robust epidemiological data on the incidence of myocardial infarction (MI) are hard to find, but synthesis of data from a number of sources indicates that the average hospital in the UK should admit about two patients with a first MI and one recurrent MI per 1000 population per year. Possibly the most relevant data on the incidence, prevalence, and persistence of post-MI heart failure can be derived from the TRACE study. Most patients will develop heart failure or major left ventricular systolic dysfunction (LVSD) at some time after an MI, most commonly during the index admission. In up to 20% of cases this will be transient, but such patients still have a poor prognosis. There is likely to be around one patient discharged per thousand population per year with heart failure or major LVSD after an acute MI. It is important to organise care structures to ensure that patients with post-MI heart failure and LVSD are identified and managed appropriately.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical