

Melioidosis: epidemiology, pathophysiology, and management
- PMID: 15831829
- PMCID: PMC1082802
- DOI: 10.1128/CMR.18.2.383-416.2005
Melioidosis: epidemiology, pathophysiology, and management
Erratum in
- Clin Microbiol Rev. 2007 Jul;20(3):533. Dosage error in article text
Abstract
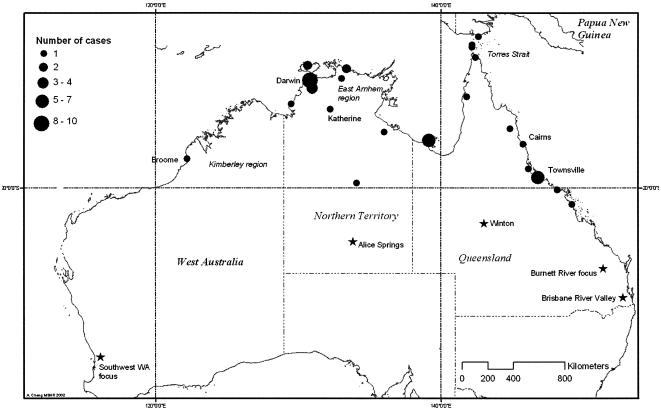
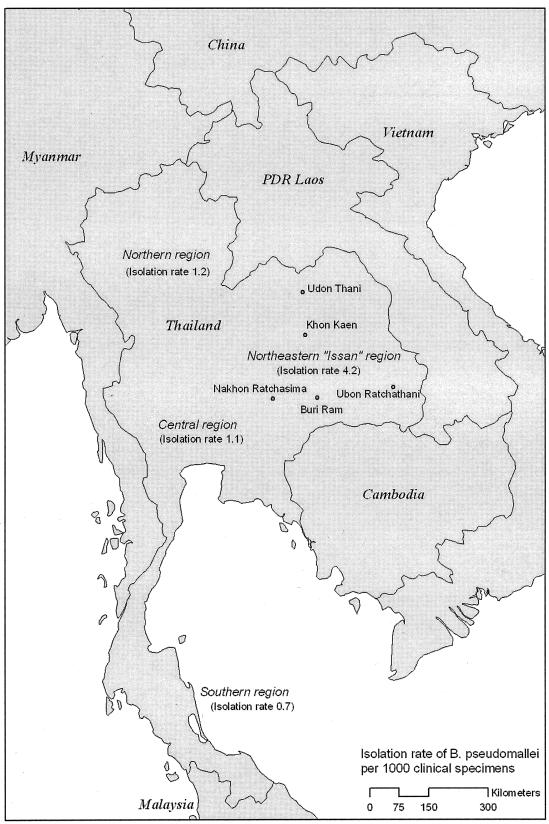
Melioidosis, caused by the gram-negative saprophyte Burkholderia pseudomallei, is a disease of public health importance in southeast Asia and northern Australia that is associated with high case-fatality rates in animals and humans. It has the potential for epidemic spread to areas where it is not endemic, and sporadic case reports elsewhere in the world suggest that as-yet-unrecognized foci of infection may exist. Environmental determinants of this infection, apart from a close association with rainfall, are yet to be elucidated. The sequencing of the genome of a strain of B. pseudomallei has recently been completed and will help in the further identification of virulence factors. The presence of specific risk factors for infection, such as diabetes, suggests that functional neutrophil defects are important in the pathogenesis of melioidosis; other studies have defined virulence factors (including a type III secretion system) that allow evasion of killing mechanisms by phagocytes. There is a possible role for cell-mediated immunity, but repeated environmental exposure does not elicit protective humoral or cellular immunity. A vaccine is under development, but economic constraints may make vaccination an unrealistic option for many regions of endemicity. Disease manifestations are protean, and no inexpensive, practical, and accurate rapid diagnostic tests are commercially available; diagnosis relies on culture of the organism. Despite the introduction of ceftazidime- and carbapenem-based intravenous treatments, melioidosis is still associated with a significant mortality attributable to severe sepsis and its complications. A long course of oral eradication therapy is required to prevent relapse. Studies exploring the role of preventative measures, earlier clinical identification, and better management of severe sepsis are required to reduce the burden of this disease.
Figures

References
-
- Abbink, F. C., J. M. Orendi, and A. J. de Beaufort. 2001. Mother-to-child transmission of Burkholderia pseudomallei. N. Engl. J. Med. 344:1171-1172. - PubMed
-
- Acute Respiratory Distress Syndrome Network. 2000. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N. Engl. J. Med. 342:1301-1308. - PubMed
-
- Ahmed, K., H. D. Enciso, H. Masaki, M. Tao, A. Omori, P. Tharavichikul, and T. Nagatake. 1999. Attachment of Burkholderia pseudomallei to pharyngeal epithelial cells: a highly pathogenic bacteria with low attachment ability. Am. J. Trop. Med. Hyg. 60:90-93. - PubMed
-
- Alejandria, M. M., M. A. Lansang, L. F. Dans, and J. B. Mantaring. 2001. Intravenous immunoglobulin for treating sepsis and septic shock (Cochrane Review). Cochrane Database Syst. Rev. 2:CD001090. - PubMed
-
- Alibek, K. 1998. Statement by Dr. Kenneth Alibek. Terrorist and intelligence operations: potential impact on the U.S. economy. Joint Economic Committee, U.S. Congress, Washington, D.C.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
