

Antibodies to carbonic anhydrase and IgG4 levels in idiopathic chronic pancreatitis: relevance for diagnosis of autoimmune pancreatitis
- PMID: 15831920
- PMCID: PMC1774474
- DOI: 10.1136/gut.2004.047142
Antibodies to carbonic anhydrase and IgG4 levels in idiopathic chronic pancreatitis: relevance for diagnosis of autoimmune pancreatitis
Abstract
Background: Increased serum antibodies against carbonic anhydrase II (CA-II Ab) or IgG4 levels have been reported in cases of autoimmune chronic pancreatitis (ACP).
Aim: To assess the relevance of serum CA-II Ab and IgG4 levels for the diagnosis of ACP in idiopathic CP (ICP) versus alcoholic CP and Sjogren's syndrome (SS).
Subjects: This was a multicentre study involving 227 subjects divided into four groups: ICP (n = 54), normal controls (n = 54, paired by age and sex with ICP patients), alcoholic CP (n = 86), and SS (n = 33).
Methods: CA-II Ab was measured by ELISA and confirmed by western blotting. A score of easy clinical use with major clinical, morphological, and biochemical parameters for the diagnosis of ACP was applied.
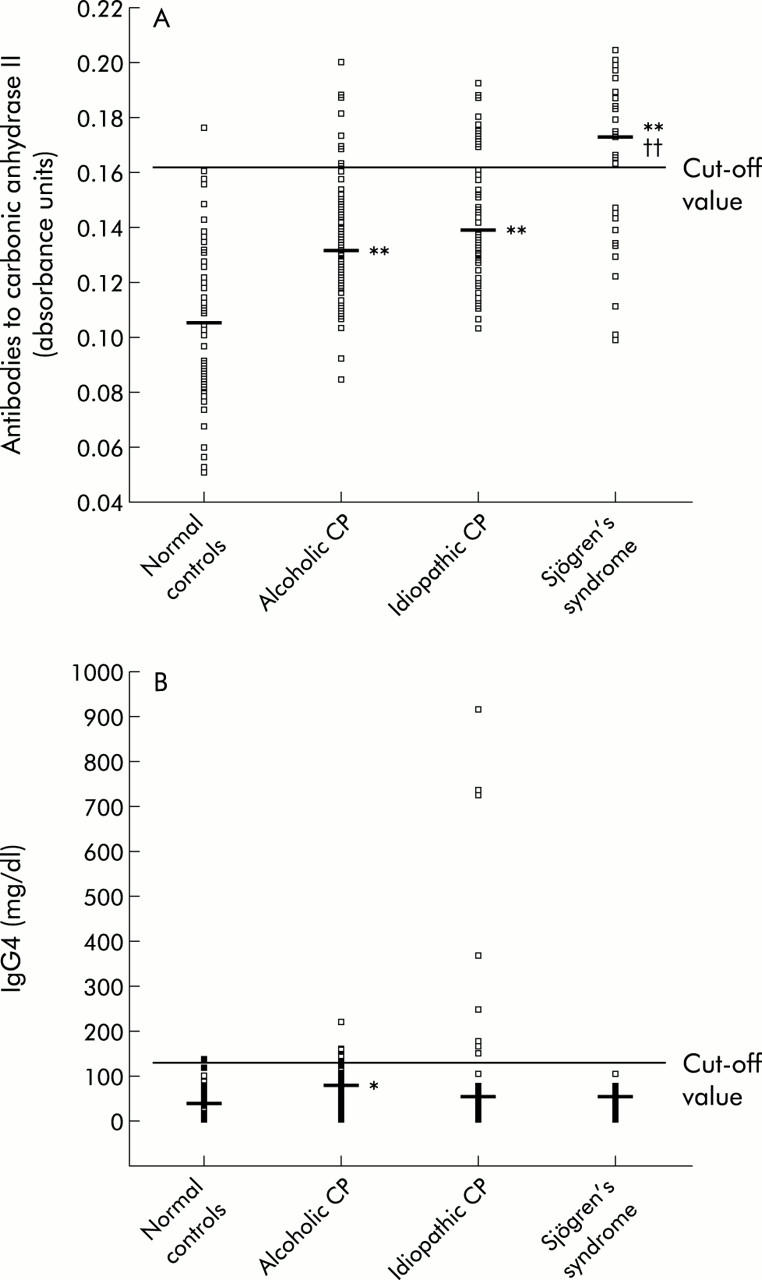
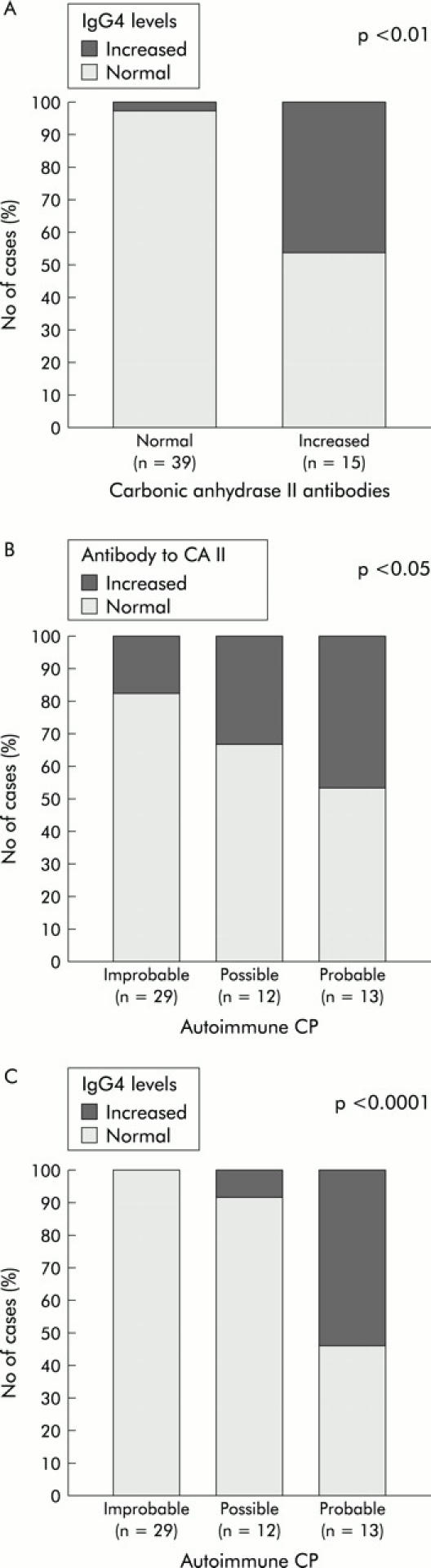
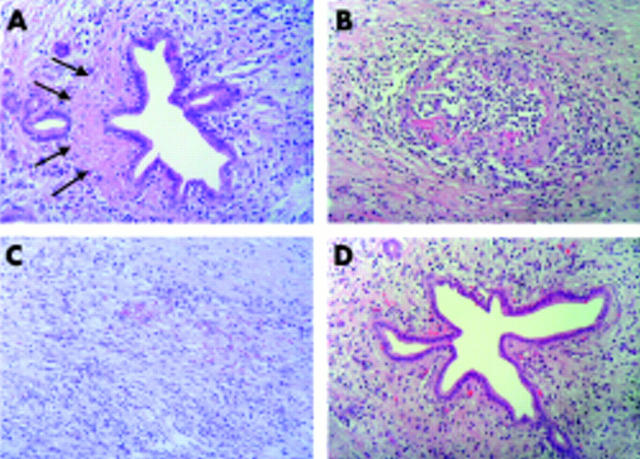
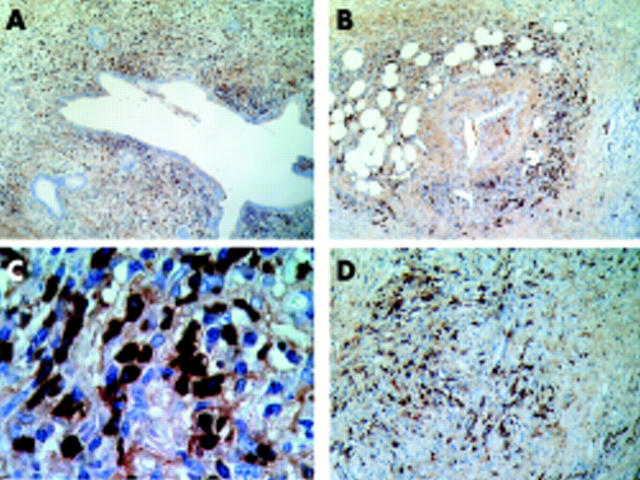
Results: The percentage of patients with increased serum CA-II Ab was higher in the ICP group (28%) than in controls (1.9%) and in patients with alcoholic CP (10.5%), but lower than in patients with SS (64%). The proportion with elevated IgG4 levels was higher in the ICP group (15%) compared with controls (1.9%) and SS (0%) but not significantly different from alcoholic CP (8%). Most ICP patients (7/8) with high IgG4 levels exhibited increased CA-II Ab and a compatible ACP score. A definitive diagnosis of ACP by histological analysis was associated with other autoimmune disorders, an increase in both serum IgG4 and CA-II Ab levels, and IgG4 positive plasma cells.
Conclusions: The increase in serum IgG4 levels was strongly associated with elevated CA-II Ab levels, manifestations compatible with ACP, and lymphoplasmacytic infiltration when surgical specimens were available.
Figures
Comment in
-
Autoimmune pancreatitis--also a Western disease.Gut. 2005 May;54(5):581-3. doi: 10.1136/gut.2004.058438. Gut. 2005. PMID: 15831898 Free PMC article. No abstract available.
References
-
- Strand V, Talal N. Advances in the diagnosis and concept of Sjögren’s syndrome (autoimmune exocrinopathy). Bull Rheum Dis 1980;30:1046–52. - PubMed
-
- Epstein O, Chapman R, Kaje-Bakaar G, et al. The pancreas in primary biliary cirrhosis and primary sclerosing cholangitis. Gastroenterology 1982;83:1177–82. - PubMed
-
- Kino-Ohsaki J, Nishimori I, Morita M, et al. Serum antibodies to carbonic anhydrase I and II in patiens with idiopatic chronic pancretitis and Sjögren’s syndrome. Gastroenteroloy 1996;110:1579–86. - PubMed
-
- Inagaki Y, Jinno-Yoshida Y, Hamasaki Y, et al. A novel autoantiboy reactive with carbonic anhydrase in sera from patients with systemic lupus erythematosus and Sjögren’s syndrome. J Dermatol Sci 1991;2:147–54. - PubMed
-
- Itoh Y, Reichlin M. Antibodies to carbonic anhydrase in systemic lupus erithematosus and other rheumatic diseases. Arthritis Rheum 1992;35:73–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous