

A prospective study of reasons for prolonged hospitalizations on a general medicine teaching service
- PMID: 15836542
- PMCID: PMC1490052
- DOI: 10.1111/j.1525-1497.2005.40269.x
A prospective study of reasons for prolonged hospitalizations on a general medicine teaching service
Abstract
Background: Delays in the care of hospitalized patients may lead to increased length of stay, iatrogenic complications, and costs. No study has characterized delays among general medicine inpatients in the current prospective payment era of care.
Objective: To quantify and characterize delays in care which prolong hospitalizations for general medicine inpatients.
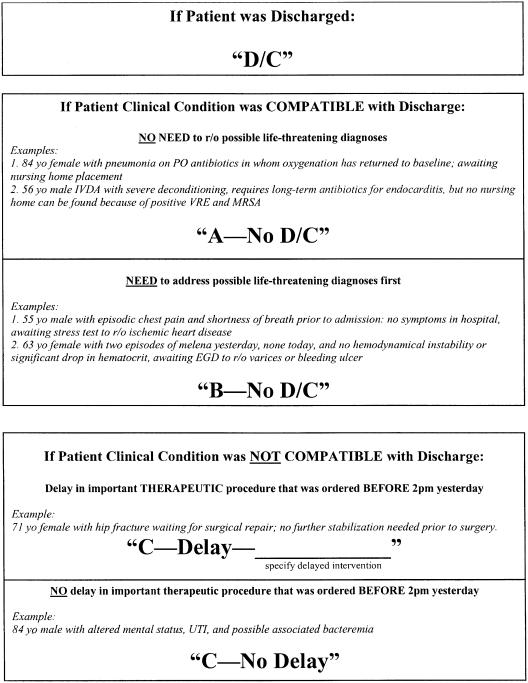
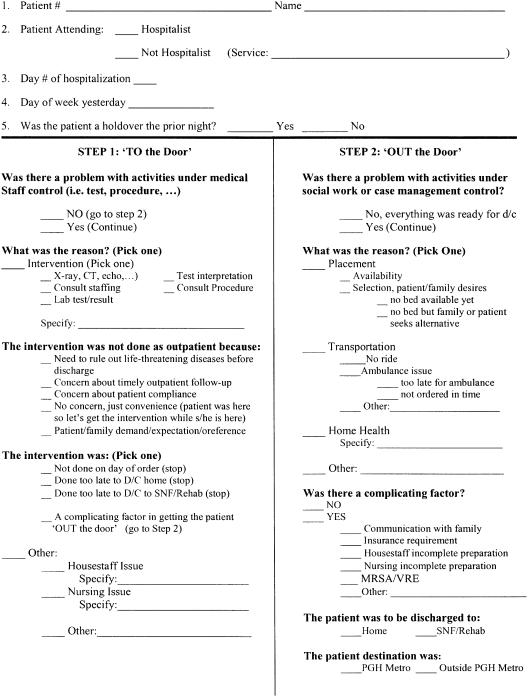
Design: Prospective survey of senior residents.
Setting: Urban tertiary care university-affiliated teaching hospital.
Participants: Sixteen senior residents were surveyed regarding 2,831 patient-days.
Interventions: None.
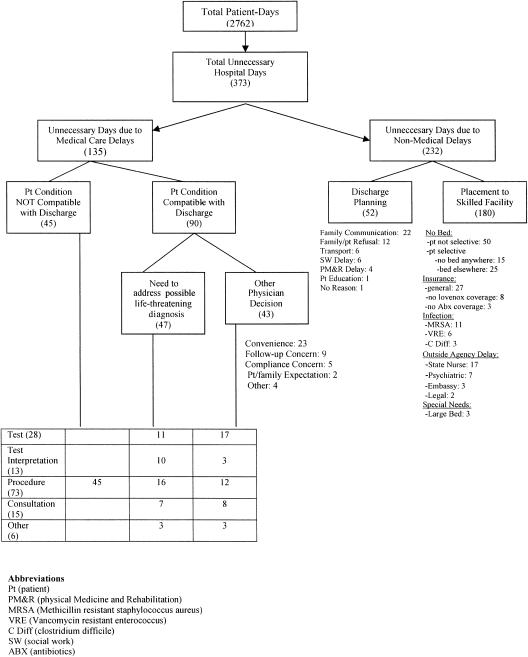
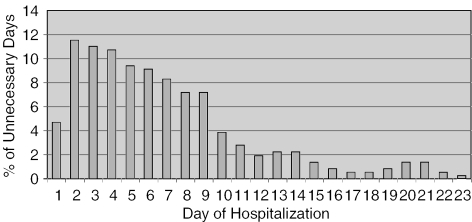
Measurements and main results: Data were collected on 97.6% (2,762) of patient-days eligible for evaluation. Three hundred seventy-three patient-days (13.5% of all hospital days) were judged unnecessary for acute inpatient care, and occurred because of delays in needed services. Sixty-three percent of these unnecessary days were due to nonmedical service delays and 37% were due to medical service delays. The vast majority of nonmedical service delays (84%) were due to difficulty finding a bed in a skilled nursing facility. Medical service delays were most often due to postponement of procedures (54%) and diagnostic test performance (21%) or interpretation (10%), and were significantly more common on weekend days (relative risk [RR], 1.49; P=.02). Indeed, nearly one fourth of unnecessary patient-days (24% overall, 88 patient-days) involved an inability to access medical services on a weekend day (Saturday or Sunday).
Conclusions: At our institution, a substantial number of hospital days were judged unnecessary for acute inpatient care and were attributable to delays in medical and nonmedical services. Future work is needed to develop and investigate measures to decrease delays.
Figures
Comment in
-
Long live generalism. Hospital medicine and the Journal of General Internal Medicine.J Gen Intern Med. 2005 Feb;20(2):208-9. doi: 10.1111/j.1525-1497.2005.41002.x. J Gen Intern Med. 2005. PMID: 15836556 Free PMC article. No abstract available.
References
-
- Braithwaite RS, Col NF, Wong JB. Estimating hip fracture morbidity, mortality, and costs. J Am Geriatr Soc. 2003;51:364–70. - PubMed
-
- Shojania KG, Duncan BW, McDonald KM, Wachter RM. Safe but sound: patient safety meets evidence-based medicine. JAMA. 2002;288:508–13. - PubMed
-
- Centers for Medicare and Medicaid Services. US Health Care System. Available at: http://www.cms.hhs.gov/charts/default.asp. Accessed January 2004.
-
- Selker HP, Beshansky JR, Pauker SG, Kassirer JP. The epidemiology of delays in a teaching hospital. Med Care. 1989;27:112–29. - PubMed
-
- Brasel KJ, Rasmussen J, Cauley C, Weigelt JA. Reasons for delayed discharge of trauma patients. J Surg Res. 2002;107:223–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical