

Vulnerability and unmet health care needs. The influence of multiple risk factors
- PMID: 15836548
- PMCID: PMC1490048
- DOI: 10.1111/j.1525-1497.2005.40136.x
Vulnerability and unmet health care needs. The influence of multiple risk factors
Abstract
Context: Previous studies have demonstrated a strong association between minority race, low socioeconomic status (SES), and lack of potential access to care (e.g., no insurance coverage and no regular source of care) and poor receipt of health care services. Most studies have examined the independent effects of these risk factors for poor access, but more practical models are needed to account for the clustering of multiple risks.
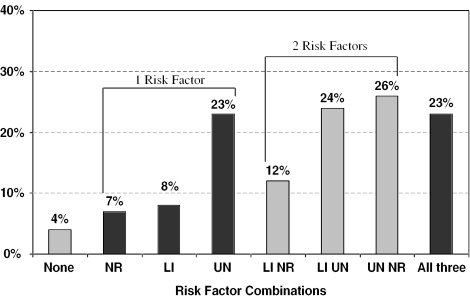
Objective: To present a profile of risk factors for poor access based on income, insurance coverage, and having a regular source of care, and examine the association of the profiles with unmet health care needs due to cost. Relationships are examined by race/ethnicity.
Design: Analysis of 32,374 adults from the 2000 National Health Interview Survey.
Main outcome measures: Reported unmet needs due to cost: missing/delaying needed medical care, and delaying obtaining prescriptions, mental health care, or dental care.
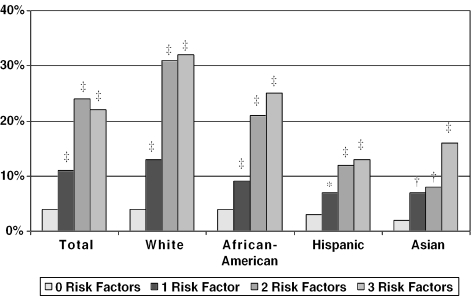
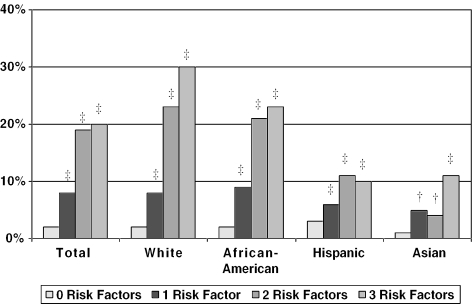
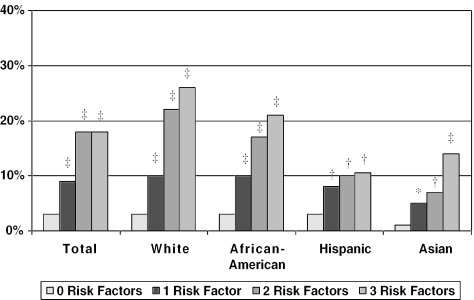
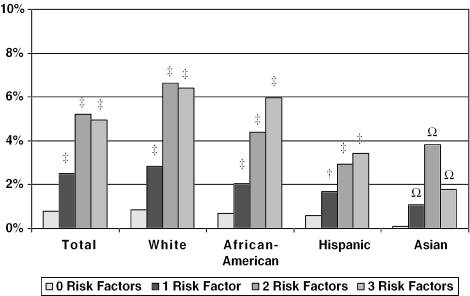
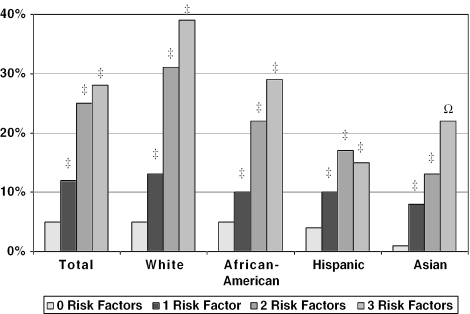
Results: Controlling for personal demographic and community factors, individuals who were low income, uninsured, and had no regular source of care were more likely to miss or delay needed health care services due to cost. After controlling for these risk factors, whites were more likely than other racial/ethnic groups to report unmet needs. When presented as a risk profile, a clear gradient existed in the likelihood of having an unmet need according to the number of risk factors, regardless of racial/ethnic group.
Conclusion: Unmet health care needs due to cost increased with higher risk profiles for each racial and ethnic group. Without attention to these co-occurring risk factors for poor access, it is unlikely that substantial reductions in disparities will be made in assuring access to needed health care services among vulnerable populations.
Figures
References
-
- Healthy People 2010. Washington, DC: U.S. Department of Health and Human Services; 2000.
-
- Smedley B, Stith A, Nelson A, editors. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington, DC: National Academy Press; 2002. - PubMed
-
- National Center for Health Statistics. Health, United States 1998, with Socioeconomic Status and Health Chartbook. Hyattsville, MD: Centers for Disease Control; 1998.
-
- Andersen R. Revisiting the behavioral model and access to medical care:does it matter? J Health Soc Behav. 1995;36:1–10. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources